

Fetal Pathology of Neural Tube Defects - An Overview of 68 Cases
- PMID: 28579621
- PMCID: PMC5444532
- DOI: 10.1055/s-0043-103459
Fetal Pathology of Neural Tube Defects - An Overview of 68 Cases
Abstract
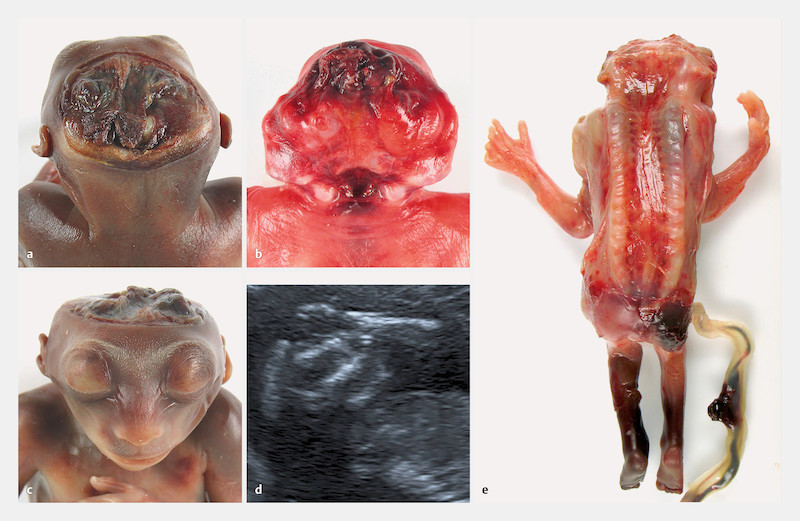
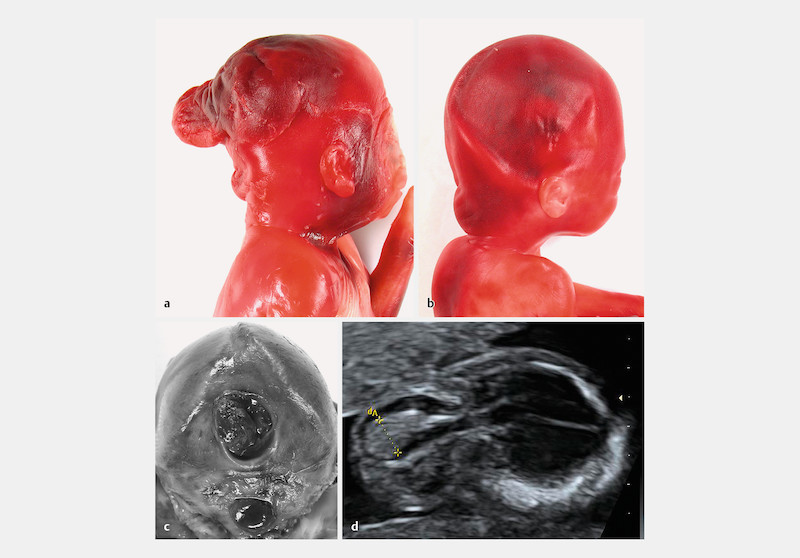
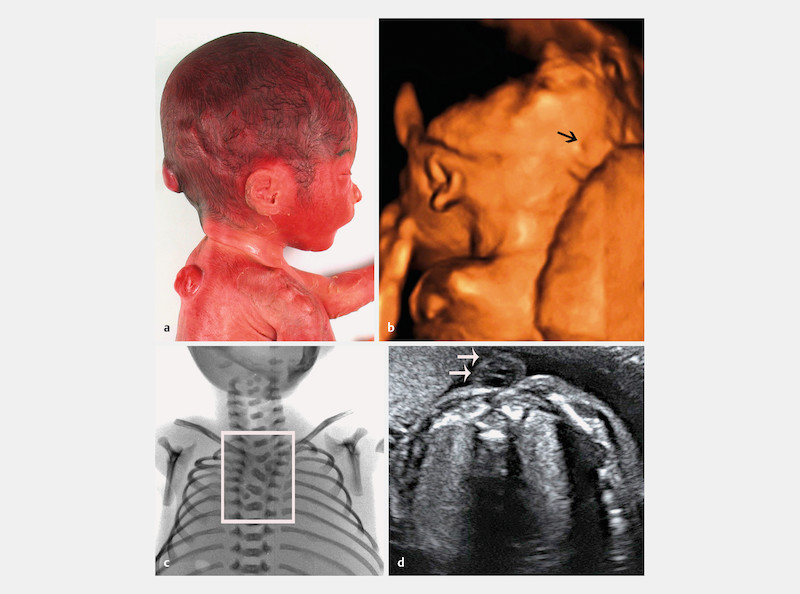
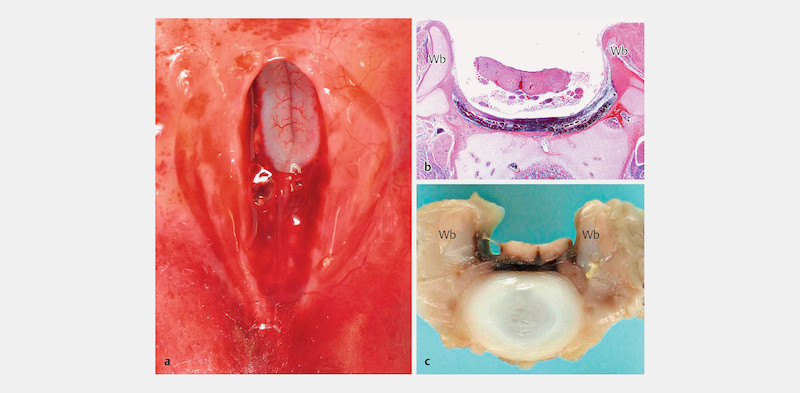
Introduction: The prevalence of neural tube defects worldwide is 1 - 2 per 1000 neonates. Neural tube defects result from a disturbance of neurulation in the 3rd or 4th week of development and thus represent the earliest manifestation of organ malformation. Neural tube defects (NTD) are classified into cranial dysraphism leading to anencephaly or meningoencephalocele and spinal dysraphism with or without meningomyelocele. In isolated form they have multifactorial causes, and the empirical risk of recurrence in Central Europe is 2%. As associated malformations they tend to occur sporadically, and in monogenic syndromes they follow Mendelian inheritance patterns with a high risk of recurrence.
Patients: Autopsies were performed on 68 fetuses following a prenatal diagnosis of NTD and induced abortion.
Results: The incidence of NTDs in our autopsied fetuses was 8% and 11% in fetuses with malformations. The percentage of fetuses with anencephaly, encephalocele or spina bifida was 24, 18, and 60%*, respectively. Analysis of the sex distribution showed a female preponderance in cranial dysraphisms but the sex distribution of spina bifida cases was equal. The extent and localization of NTDs varied, with lumbosacral cases clearly predominating. The proportion of isolated, associated and syndromic neural tube defects was 56, 23.5 and 20.6% respectively. In the majority of syndromes, the neural tube defect represented a not previously observed syndromic feature.
Conclusion: The high proportion of NTDs with monogenic background underlines the importance of a syndrome oriented fetal pathology. At the very least it requires a thourough photographic and radiographic documentation of the fetal phenotype to enable the genetic counsellor to identify a syndromic disorder. This is necessary to determine the risk of recurrence, arrange confirming mutation analyses and offer targeted prenatal diagnosis in subsequent pregnancies.
Einleitung Neuralrohrdefekte zeigen weltweit eine Prävalenz von 1 – 2 : 1000 unter Neugeborenen. Sie beruhen auf einer gestörten Neurulation in der 3. – 4. Entwicklungswoche und stellen damit die früheste Manifestation einer Organfehlbildung dar. Neuralrohrdefekte lassen sich in kraniale Dysraphien mit Anenzephalie oder Meningoenzephalozele und spinale Dysraphien mit oder ohne Meningomyelozele einteilen. In isolierter Form sind sie multifaktoriell bedingt und in Mitteleuropa mit einem empirischen Wiederholungsrisiko von 2% behaftet. Als assoziierte Fehlbildung treten sie zumeist sporadisch auf und in monogenen Syndromen folgen sie einem Mendel-Erbgang mit hohem Wiederholungsrisiko. Patienten Die Untersuchungen erfolgten an 68 Feten, die uns nach Pränataldiagnose eines Neuralrohrdefekts und Schwangerschaftsabbruch zur Obduktion überstellt worden waren. Ergebnisse Die Rate von Neuralrohrdefekten in unserem fetalpathologischen Obduktionsgut betrug 8%, bezogen auf die Feten mit Fehlbildungen 11%. Der Anteil der Anenzephalien, Enzephalozelen und Spinae bifidae lag bei 24 : 18 : 60%*. Das Geschlechtsverhältnis ergab eine deutliche Bevorzugung des weiblichen Geschlechts bei den kranialen Dysraphien und war ausgeglichen unter den Spina-bifida-Fällen. Die Neuralrohrdefekte variierten in Ausdehnung und Lokalisation. In der großen Mehrzahl der Fälle waren sie lumbosakral gelegen. Isolierte, assoziierte und syndromale Neuralrohrdefekte traten mit einer Häufigkeit von 56 : 23,5 : 20,6% auf. Bei der Mehrzahl der Syndrome stellte der Neuralrohrdefekt ein bisher nicht beobachtetes Merkmal dar. Schlussfolgerungen Eine syndromorientierte fetalpathologische Untersuchung oder zumindest eine fotografische und röntgenologische Dokumentation des fetalen Phänotyps zur Syndromerkennung durch den genetischen Berater sind die Voraussetzungen für die Bestimmung des Wiederholungsrisikos und eine gezielte pränatale Diagnostik bei nachfolgenden Schwangerschaften.
Keywords: Chiari II malformation; encephalocele; fetal pathology; neural tube defects; spina bifida.
Conflict of interest statement
Die Autoren erklären, dass bei der Erstellung des Beitrags keine Interessenkonflikte im Sinne der Empfehlungen des International Commitee of Medical Journal Editors bestanden.
Figures


Similar articles
-
Spina bifida and other neural tube defects.Curr Probl Pediatr. 2000 Nov-Dec;30(10):313-32. doi: 10.1067/mpp.2000.112052. Curr Probl Pediatr. 2000. PMID: 11147289 Review.
-
Trends in neural tube defects 1980-1989.Med J Aust. 1993 Feb 1;158(3):152-4. doi: 10.5694/j.1326-5377.1993.tb121690.x. Med J Aust. 1993. PMID: 8450777
-
Neural tube defects in the sample of genetic counselling.Prenat Diagn. 2007 Oct;27(10):912-21. doi: 10.1002/pd.1801. Prenat Diagn. 2007. PMID: 17602445
-
Surveillance for anencephaly and spina bifida and the impact of prenatal diagnosis--United States, 1985-1994.MMWR CDC Surveill Summ. 1995 Aug 25;44(4):1-13. MMWR CDC Surveill Summ. 1995. PMID: 7637675
-
Etiology, pathogenesis and prevention of neural tube defects.Congenit Anom (Kyoto). 2006 Jun;46(2):55-67. doi: 10.1111/j.1741-4520.2006.00104.x. Congenit Anom (Kyoto). 2006. PMID: 16732763 Review.
Cited by
-
Cerebral Abnormalities in Spina Bifida: A Neuropathological Study.Pediatr Dev Pathol. 2022 Mar-Apr;25(2):107-123. doi: 10.1177/10935266211040500. Epub 2021 Oct 6. Pediatr Dev Pathol. 2022. PMID: 34614376 Free PMC article.
-
Smith-Lemli-Opitz syndrome - Fetal phenotypes with special reference to the syndrome-specific internal malformation pattern.Birth Defects Res. 2020 Jan 15;112(2):175-185. doi: 10.1002/bdr2.1620. Epub 2019 Dec 16. Birth Defects Res. 2020. PMID: 31840946 Free PMC article.
-
Open Spinal Dysraphism Without Hindbrain Herniation-Natural History and Postnatal Outcome.Prenat Diagn. 2025 Aug;45(9):1106-1114. doi: 10.1002/pd.6855. Epub 2025 Jul 8. Prenat Diagn. 2025. PMID: 40627407 Free PMC article.
-
Prenatal phenotype of PNKP-related primary microcephaly associated with variants affecting both the FHA and phosphatase domain.Eur J Hum Genet. 2022 Jan;30(1):101-110. doi: 10.1038/s41431-021-00982-y. Epub 2021 Oct 25. Eur J Hum Genet. 2022. PMID: 34697416 Free PMC article.
-
Piepkorn type of osteochondrodysplasia: Defining the severe end of FLNB-related skeletal disorders in three fetuses and a 106-year-old exhibit.Am J Med Genet A. 2018 Jul;176(7):1559-1568. doi: 10.1002/ajmg.a.38828. Epub 2018 May 23. Am J Med Genet A. 2018. PMID: 29797497 Free PMC article.
References
-
- Larsen W. 3rd ed. Philadelphia: Churchill Livingstone; 2001. Human Embryology; pp. 98–102.
-
- Bassuk A G, Kibar Z. Genetic basis of neural tube defects. Semin Pediatr Neurol. 2009;16:101–110. - PubMed
-
- Kibar Z, Torban E, McDearmid J R. Mutations in VANGL1 associated with neural-tube defects. N Engl J Med. 2007;356:1432–1437. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials