

Metastatic Liver Disease: Indications for Locoregional Therapy and Supporting Data
- PMID: 28579683
- PMCID: PMC5453777
- DOI: 10.1055/s-0037-1602712
Metastatic Liver Disease: Indications for Locoregional Therapy and Supporting Data
Abstract
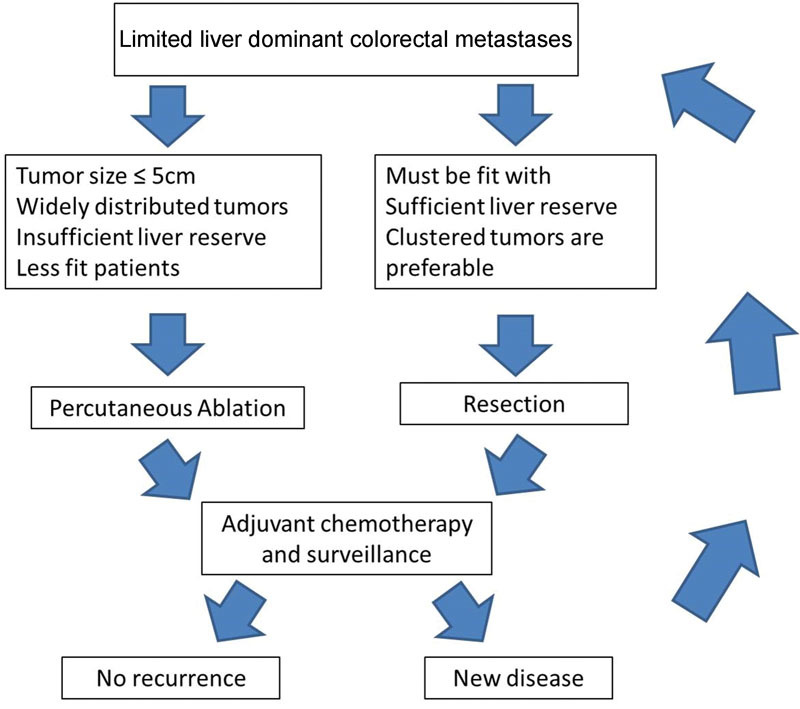
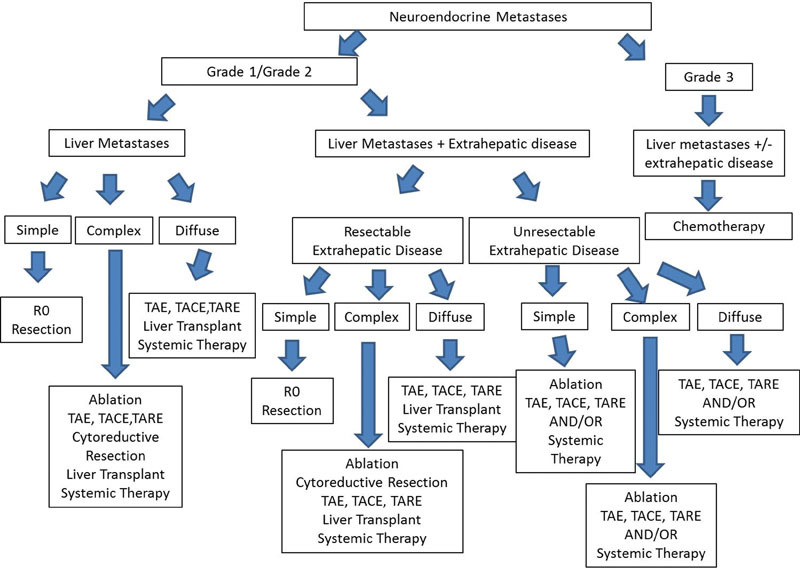
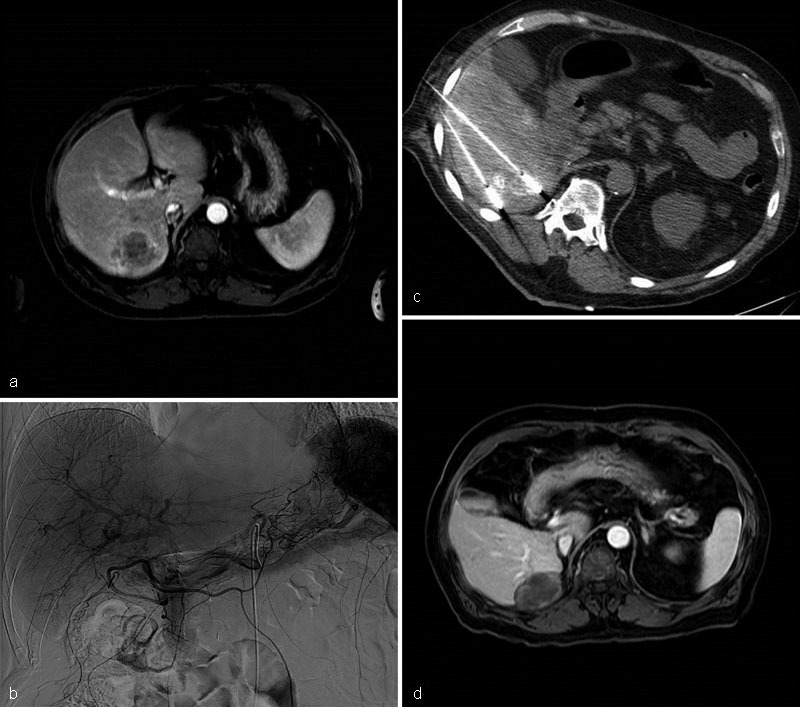
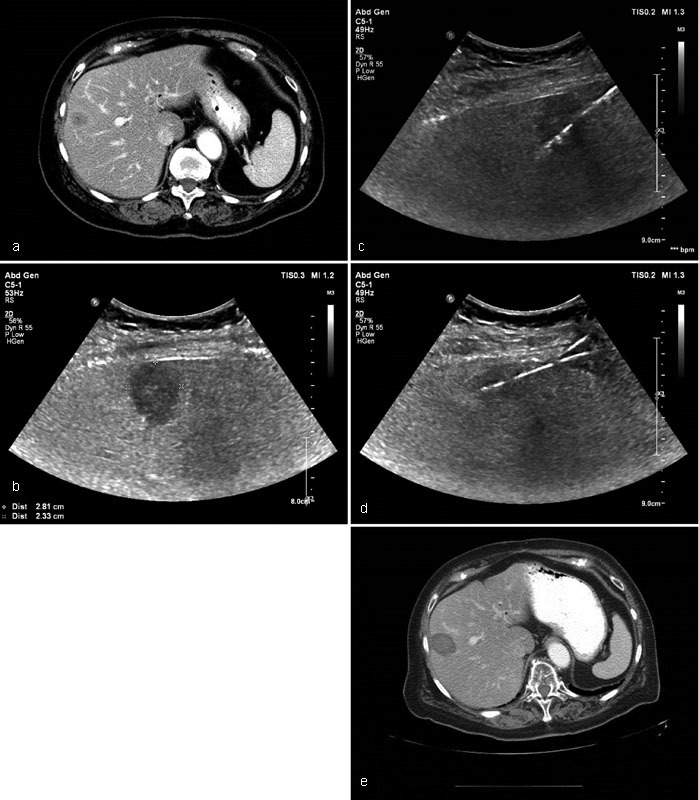
Metastatic liver disease is a major cause of cancer-related morbidity and mortality. Surgical resection is considered the only curative treatment, yet only a minority is eligible. Patients who present with unresectable disease are treated with systemic agents and/or locoregional therapies. The latter include thermal ablation and catheter-based transarterial interventions. Thermal ablation is reserved for those with limited tumor burden. It is used to downstage the disease to enable curative surgical resection, as an adjunct to surgery, or in select patients it is potentially curative. Transarterial therapies are indicated in those with more diffuse disease. The goals of care are to palliate symptoms and prolong survival. The indications and supporting data for thermal ablation and transarterial interventions are reviewed, technical and tumor factors that need to be considered prior to intervention are outlined, and finally several cases are presented.
Keywords: chemoembolization; interventional radiology; liver metastases; locoregional therapy; radioembolization; thermal ablation.
Figures
References
-
- Robinson P J. Imaging liver metastases: current limitations and future prospects. Br J Radiol. 2000;73(867):234–241. - PubMed
-
- Jemal A, Murray T, Ward E et al.Cancer statistics, 2005. CA Cancer J Clin. 2005;55(01):10–30. - PubMed
-
- Forner A, Llovet J M, Bruix J.Hepatocellular carcinoma Lancet 2012379(9822):1245–1255. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
