

Acute mechanical circulatory support for cardiogenic shock: the "door to support" time
- PMID: 28580136
- PMCID: PMC5443341
- DOI: 10.12688/f1000research.11150.1
Acute mechanical circulatory support for cardiogenic shock: the "door to support" time
Abstract
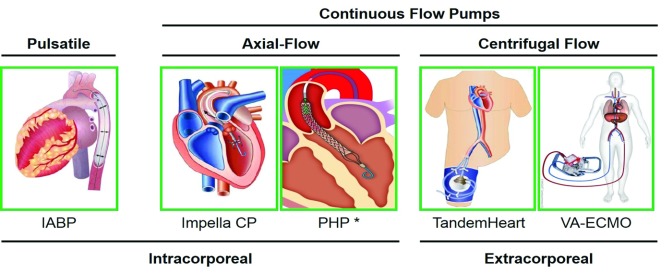
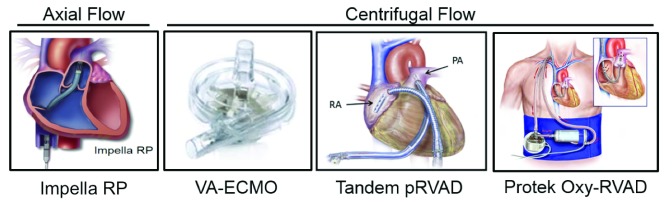
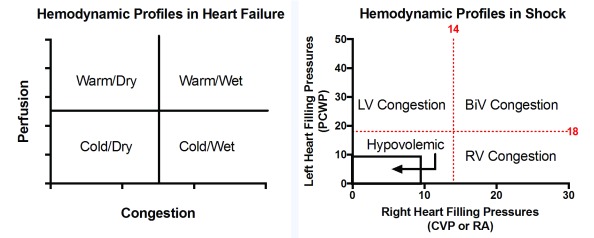
Cardiogenic shock (CS) remains a major cause of in-hospital mortality in the setting of acute myocardial infarction. CS begins as a hemodynamic problem with impaired cardiac output leading to reduced systemic perfusion, increased residual volume within the left and right ventricles, and increased cardiac filling pressures. A critical step towards the development of future algorithms is a clear understanding of the treatment objectives for CS. In this review, we introduce the "door to support" time as an emerging target of therapy to improve outcomes associated with CS, define four key treatment objectives in the management of CS, discuss the importance of early hemodynamic assessment and appropriate selection of acute mechanical circulatory support (AMCS) devices for CS, and introduce a classification scheme that identifies subtypes of CS based on cardiac filling pressures.
Keywords: acute mechanical circulatory support; cardiogenic shock; hemodynamics; percutaneous ventricular assist device; ventricular unloading.
Conflict of interest statement
Competing interests: Navin Kapur receives research support, consulting fees, and speaker honoraria from Abiomed Inc, Maquet-Getinge Inc, Abbott Inc, and CardiacAssist Inc. Michele Esposito declares that she has no competing interests.No competing interests were disclosed.No competing interests were disclosed.Competing interests: Unrestricted institutional educational grant from Abiomed and Consultant to HeartWare Division of Medtronic
Figures

References
-
- Wayangankar SA, Bangalore S, McCoy LA, et al. : Temporal Trends and Outcomes of Patients Undergoing Percutaneous Coronary Interventions for Cardiogenic Shock in the Setting of Acute Myocardial Infarction: A Report From the CathPCI Registry. JACC Cardiovasc Interv. 2016;9(4):341–51. 10.1016/j.jcin.2015.10.039 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources