

Effects of Acute-Postacute Continuity on Community Discharge and 30-Day Rehospitalization Following Inpatient Rehabilitation
- PMID: 28580725
- PMCID: PMC5583304
- DOI: 10.1111/1475-6773.12678
Effects of Acute-Postacute Continuity on Community Discharge and 30-Day Rehospitalization Following Inpatient Rehabilitation
Abstract
Objective: To examine the effects of facility-level acute-postacute continuity on probability of community discharge and 30-day rehospitalization following inpatient rehabilitation.
Data sources: We used national Medicare enrollment, claims, and assessment data to study 541,097 patients discharged from 1,156 inpatient rehabilitation facilities (IRFs) in 2010-2011.
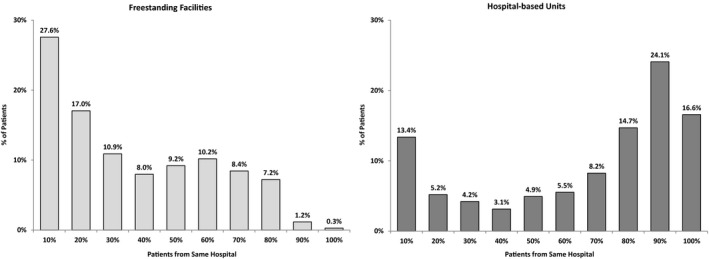
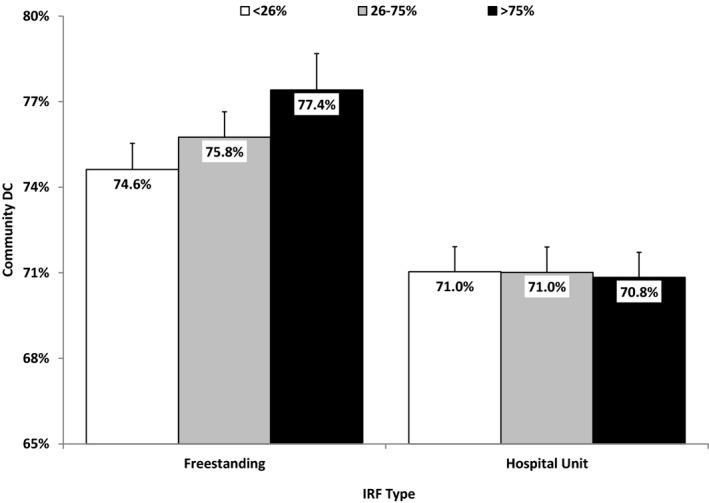
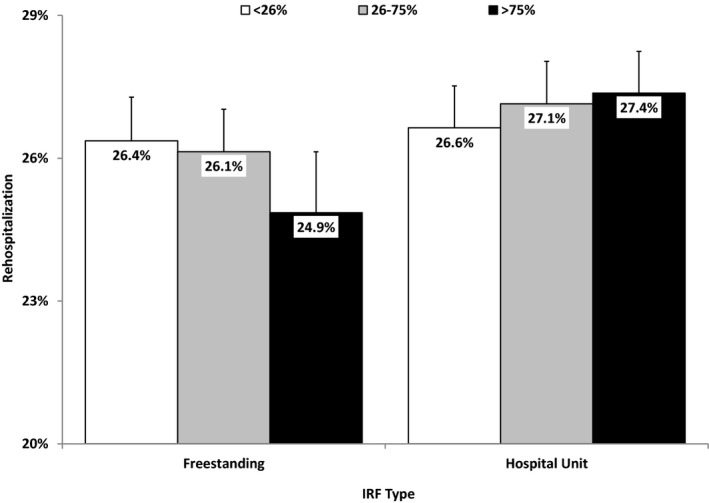
Study design: We calculated facility-level continuity as the percentages of an IRF's patients admitted from each contributing acute care hospital. Patients were categorized into three groups: low continuity (<26 percent from same hospital that discharged the patient), medium continuity (26-75 percent from same hospital), or high continuity (>75 percent from same hospital). The multivariable models included an interaction term to examine the potential moderating effects of facility type (freestanding facility vs. hospital-based rehabilitation unit) on the relationships between facility-level continuity and our two outcomes: community discharge and 30-day rehospitalization.
Principal findings: Medicare beneficiaries in hospital-based rehabilitation units were more likely to be referred from a high-contributing hospital compared to those in freestanding facilities. However, the association between higher acute-postacute continuity and desirable outcomes is significantly better in freestanding rehabilitation facilities than in hospital-based units.
Conclusions: Improving continuity is a key premise of health care reform. We found that both observed referral patterns and continuity-related benefits differed markedly by facility type. These findings provide a starting point for health systems establishing or strengthening acute-postacute relationships to improve patient outcomes in this new era of shared accountability and public quality reporting programs.
Keywords: Medicare; Referrals and referral networks; hospitals; quality of care/patient safety (measurement); rehabilitation services.
© Health Research and Educational Trust.
Figures
Comment in
-
Response to "Relationships between Acute and Postacute Care Providers: Measurement and Estimation".Health Serv Res. 2017 Oct;52(5):1629-1630. doi: 10.1111/1475-6773.12707. Epub 2017 Jun 5. Health Serv Res. 2017. PMID: 28580588 Free PMC article. No abstract available.
-
Relationships between Acute and Postacute Care Providers: Measurement and Estimation.Health Serv Res. 2017 Oct;52(5):1621-1628. doi: 10.1111/1475-6773.12715. Epub 2017 Jun 5. Health Serv Res. 2017. PMID: 28580644 Free PMC article. No abstract available.
References
-
- Bingenheimer, J. B. , and Raudenbush S. W.. 2004. “Statistical and Substantive Inferences in Public Health: Issues in the Application of Multilevel Models.” Annual Review of Public Health 25: 53–77. - PubMed
-
- Centers for Medicare & Medicaid Services . (2016). “List of Measures Under Consideration” [accessed on December 1, 2016]. Available at http://www.qualityforum.org/Project_Pages/MAP_Coordinating_Committee.aspx
-
- Chen, L. M. , and Ayanian J. Z.. 2014. “Care Continuity and Care Coordination: What Counts?” JAMA Internal Medicine 174 (5): 749–50. - PubMed
-
- Donaldson, M. S. 2001. “Continuity of Care: A Reconceptualization.” Medical Care Research and Review 58 (3): 255–90. - PubMed
-
- Elixhauser, A. , Steiner C., Harris D. R., and Coffey R. M.. 1998. “Comorbidity Measures for Use with Administrative Data.” Medical Care 36 (1): 8–27. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
