

Improving Recognition of Pediatric Severe Sepsis in the Emergency Department: Contributions of a Vital Sign-Based Electronic Alert and Bedside Clinician Identification
- PMID: 28583403
- PMCID: PMC5698118
- DOI: 10.1016/j.annemergmed.2017.03.019
Improving Recognition of Pediatric Severe Sepsis in the Emergency Department: Contributions of a Vital Sign-Based Electronic Alert and Bedside Clinician Identification
Abstract
Study objective: Recognition of pediatric sepsis is a key clinical challenge. We evaluate the performance of a sepsis recognition process including an electronic sepsis alert and bedside assessment in a pediatric emergency department (ED).
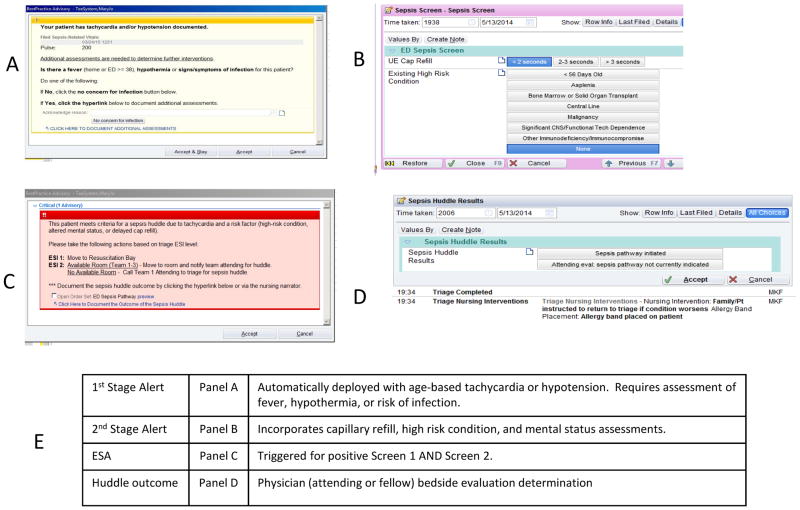
Methods: This was a cohort study with quality improvement intervention in a pediatric ED. Exposure was a positive electronic sepsis alert, defined as elevated pulse rate or hypotension, concern for infection, and at least one of the following: abnormal capillary refill, abnormal mental status, or high-risk condition. A positive electronic sepsis alert prompted team assessment or huddle to determine need for sepsis protocol. Clinicians could initiate team assessment or huddle according to clinical concern without positive electronic sepsis alert. Severe sepsis outcome defined as activation of the sepsis protocol in the ED or development of severe sepsis requiring ICU admission within 24 hours.
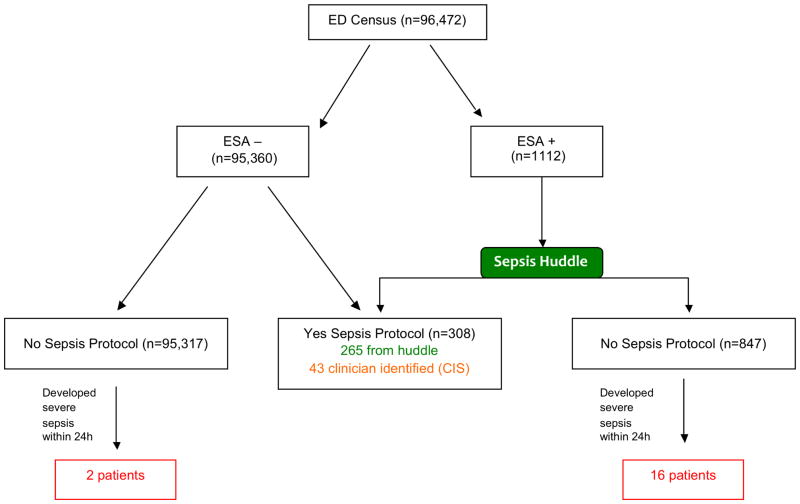
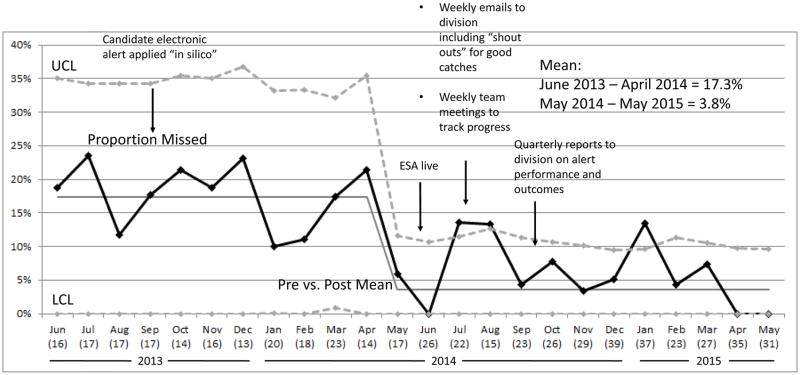
Results: There were 182,509 ED visits during the study period, with 86,037 before electronic sepsis alert implementation and 96,472 afterward, and 1,112 (1.2%) positive electronic sepsis alerts. Overall, 326 patients (0.3%) were treated for severe sepsis within 24 hours. Test characteristics of the electronic sepsis alert alone to detect severe sepsis were sensitivity 86.2% (95% confidence interval [CI] 82.0% to 89.5%), specificity 99.1% (95% CI 99.0% to 99.2%), positive predictive value 25.4% (95% CI 22.8% to 28.0%), and negative predictive value 100% (95% CI 99.9% to 100%). Inclusion of the clinician screen identified 43 additional electronic sepsis alert-negative children, with severe sepsis sensitivity 99.4% (95% CI 97.8% to 99.8%) and specificity 99.1% (95% CI 99.1% to 99.2%). Electronic sepsis alert implementation increased ED sepsis detection from 83% to 96%.
Conclusion: Electronic sepsis alert for severe sepsis demonstrated good sensitivity and high specificity. Addition of clinician identification of electronic sepsis alert-negative patients further improved sensitivity. Implementation of the electronic sepsis alert was associated with improved recognition of severe sepsis.
Copyright © 2017 American College of Emergency Physicians. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Between the Devil and the Deep Blue Sea: Use of Real-Time Tools to Identify Children With Severe Sepsis in the Pediatric Emergency Department.Ann Emerg Med. 2017 Dec;70(6):769-770. doi: 10.1016/j.annemergmed.2017.04.006. Epub 2017 Jun 2. Ann Emerg Med. 2017. PMID: 28583402 No abstract available.
References
-
- Balamuth F, Carr B, Kallan MJ, Alpern E. Pediatric Academic Societies. Vancouver; British Columbia, Canada: 2014. Epidemiology and Outcomes of Pediatric Sepsis in the United States.
-
- Hartman ME, Linde-Zwirble WT, Angus DC, Watson RS. Trends in the Epidemiology of Pediatric Severe Sepsis. Pediatr Crit Care Med. 2013 Jul 26; - PubMed
-
- Carcillo JA, Fields AI. Clinical practice parameters for hemodynamic support of pediatric and neonatal patients in septic shock. Crit Care Med. 2002 Jun;30(6):1365–1378. - PubMed
-
- Goldstein B, Giroir B, Randolph A. International pediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in pediatrics. Pediatr Crit Care Med. 2005 Jan;6(1):2–8. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
