

Phenotypic and genetic aspects of epithelial barrier function in asthmatic patients
- PMID: 28583446
- PMCID: PMC5457128
- DOI: 10.1016/j.jaci.2017.04.005
Phenotypic and genetic aspects of epithelial barrier function in asthmatic patients
Abstract
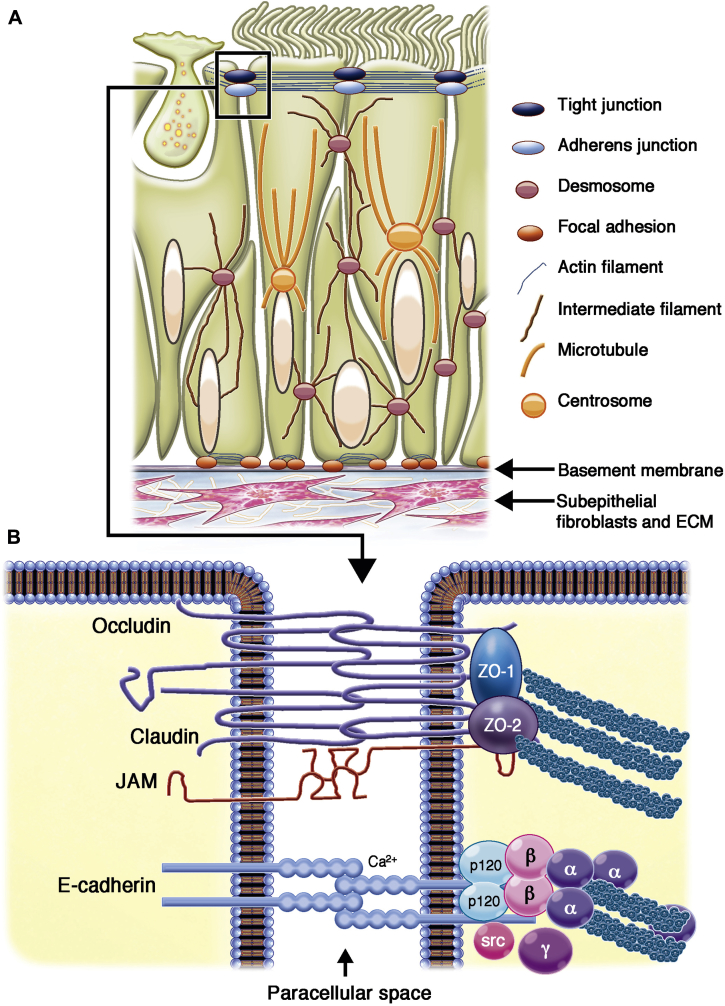
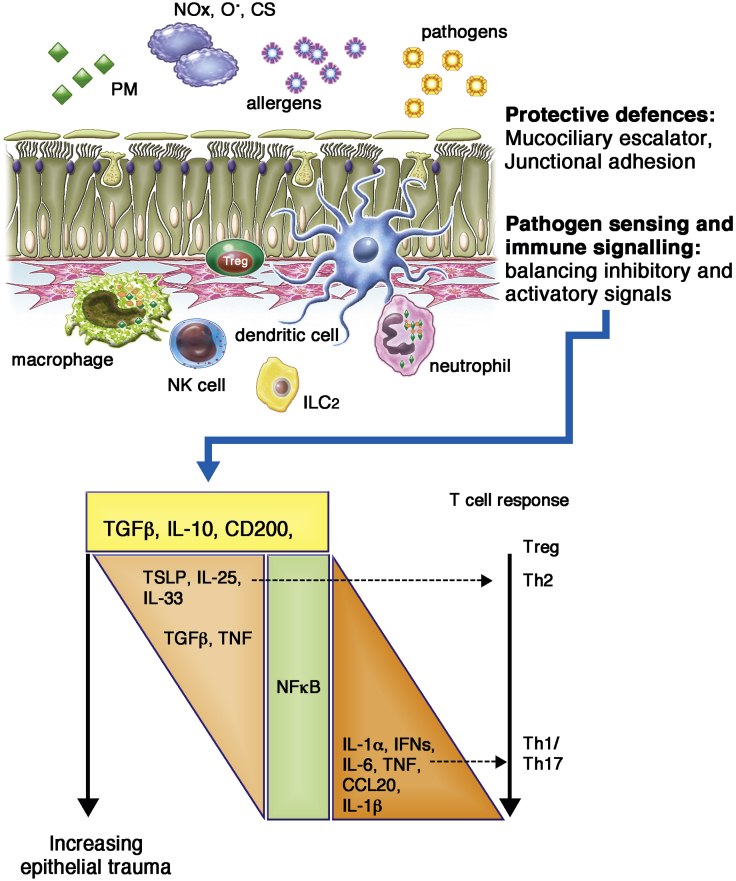
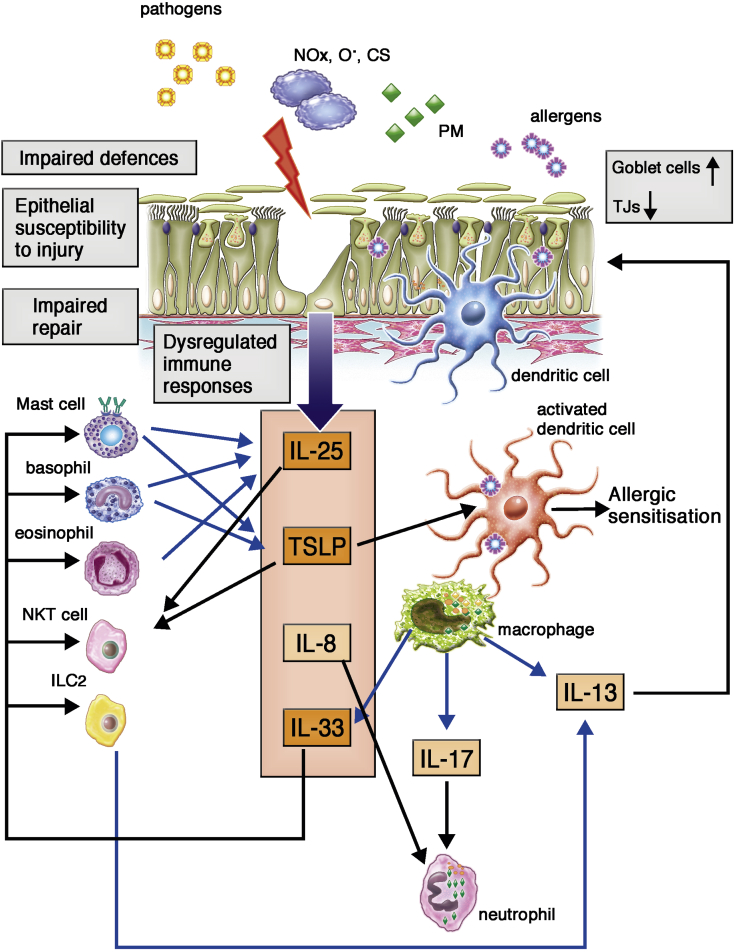
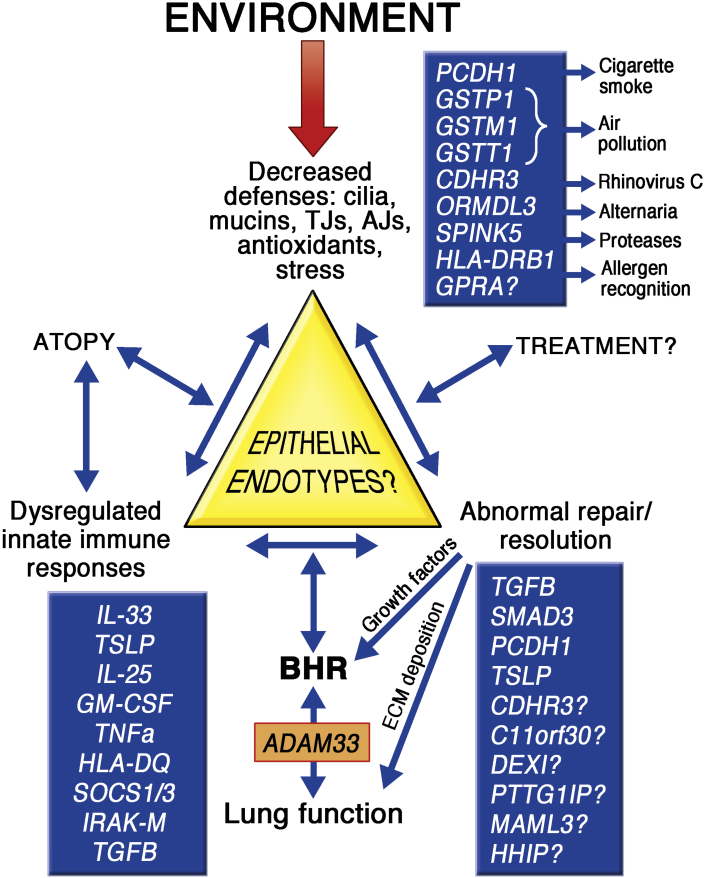
The bronchial epithelium is continuously exposed to a multitude of noxious challenges in inhaled air. Cellular contact with most damaging agents is reduced by the action of the mucociliary apparatus and by formation of a physical barrier that controls passage of ions and macromolecules. In conjunction with these defensive barrier functions, immunomodulatory cross-talk between the bronchial epithelium and tissue-resident immune cells controls the tissue microenvironment and barrier homeostasis. This is achieved by expression of an array of sensors that detect a wide variety of viral, bacterial, and nonmicrobial (toxins and irritants) agents, resulting in production of many different soluble and cell-surface molecules that signal to cells of the immune system. The ability of the bronchial epithelium to control the balance of inhibitory and activating signals is essential for orchestrating appropriate inflammatory and immune responses and for temporally modulating these responses to limit tissue injury and control the resolution of inflammation during tissue repair. In asthmatic patients abnormalities in many aspects of epithelial barrier function have been identified. We postulate that such abnormalities play a causal role in immune dysregulation in the airways by translating gene-environment interactions that underpin disease pathogenesis and exacerbation.
Keywords: Asthma; cytokine; homeostasis; innate immunity; tight junction.
Copyright © 2017 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Muraro A., Lemanske R.F., Jr., Hellings P.W., Akdis C.A., Bieber T., Casale T.B. Precision medicine in patients with allergic diseases: airway diseases and atopic dermatitis—PRACTALL document of the European Academy of Allergy and Clinical Immunology and the American Academy of Allergy, Asthma & Immunology. J Allergy Clin Immunol. 2016;137:1347–1358. - PubMed
-
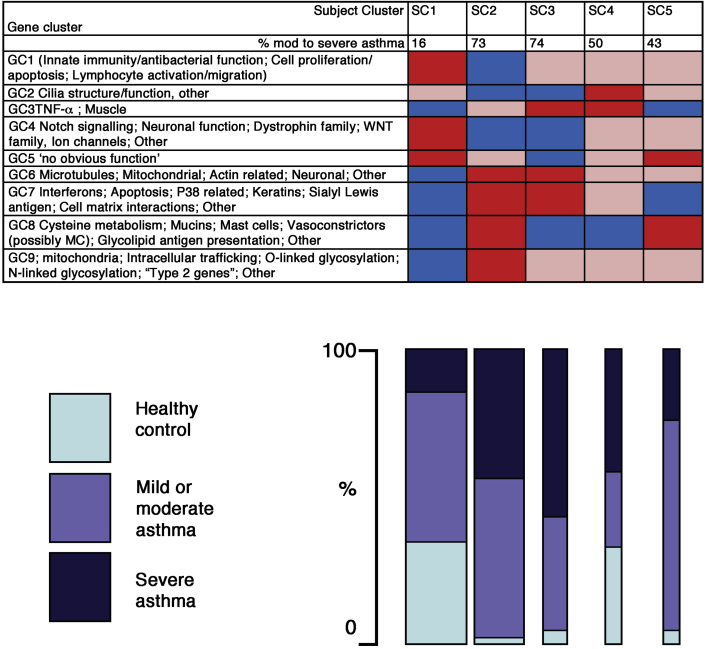
- Loza M.J., Adcock I., Auffray C., Chung K.F., Djukanovic R., Sterk P.J. Longitudinally stable, clinically defined clusters of patients with asthma independently identified in the ADEPT and U-BIOPRED asthma studies. Ann Am Thorac Soc. 2016;13(suppl 1):S102–S103. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
