

Vaginal birth after two previous caesarean deliveries in a patient with uterus didelphys and an interuterine septal defect
- PMID: 28584004
- PMCID: PMC5534647
- DOI: 10.1136/bcr-2016-219149
Vaginal birth after two previous caesarean deliveries in a patient with uterus didelphys and an interuterine septal defect
Abstract
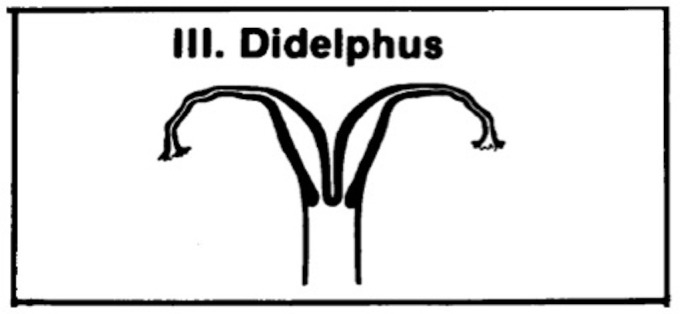
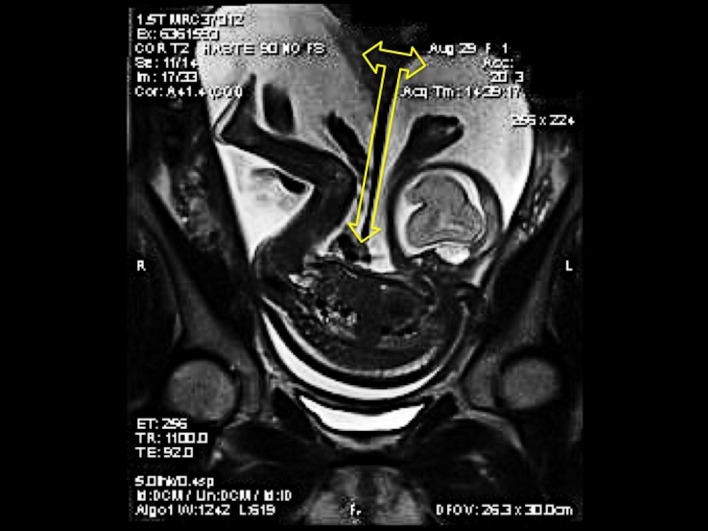
Uterus didelphys is a congenital abnormality characterised by double uteri, double cervices and a double or single vagina that affects 0.3% to 11% of the general female population. A 23-year-old woman, gravida 3 para 3003, with uterus didelphys, acquired an iatrogenic interuterine septal defect during an otherwise routine primary caesarean delivery for fetal malpresentation. The defect was repaired but noted to have dehisced during her second pregnancy. A repeat caesarean section was performed due to fetal malpresentation after an unsuccessful external cephalic version. The dehisced defect was left unrepaired. During her third pregnancy, the placenta implanted in the right uterus, but the fetus migrated to the left uterus at approximately 28 weeks gestation. The umbilical cord traversed the interuterine septal defect. With the fetus in the vertex presentation at term gestation, the patient underwent a vaginal birth after two previous caesarean deliveries without any major perinatal complications.
Keywords: obstetrics and gynaecology; pregnancy.
© BMJ Publishing Group Ltd (unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Successful external cephalic version in a patient with uterus didelphys and fetal malpresentation.BMJ Case Rep. 2019 Nov 19;12(11):e230965. doi: 10.1136/bcr-2019-230965. BMJ Case Rep. 2019. PMID: 31748355 Free PMC article.
-
Pregnancy and Childbirth in Uterus Didelphys: A Report of Three Cases.Medicina (Kaunas). 2020 Apr 23;56(4):198. doi: 10.3390/medicina56040198. Medicina (Kaunas). 2020. PMID: 32340393 Free PMC article.
-
Management of a twin pregnancy in a didelphys uterus: one fetus in each uterine cavity.BMJ Case Rep. 2020 Aug 25;13(8):e235256. doi: 10.1136/bcr-2020-235256. BMJ Case Rep. 2020. PMID: 32843451 Free PMC article.
-
Uterus didelphys: Anatomic variant.J Med Imaging Radiat Oncol. 2018 Oct;62 Suppl 1:115. doi: 10.1111/1754-9485.58_12784. J Med Imaging Radiat Oncol. 2018. PMID: 30309100 Review. No abstract available.
-
SOGC clinical practice guidelines. Guidelines for vaginal birth after previous caesarean birth. Number 155 (Replaces guideline Number 147), February 2005.Int J Gynaecol Obstet. 2005 Jun;89(3):319-31. doi: 10.1016/j.ijgo.2005.03.015. Int J Gynaecol Obstet. 2005. PMID: 16001462 Review.
Cited by
-
Successful Vaginal Delivery after External Cephalic Version in a Woman with a Large Partial Uterine Septum.Case Rep Obstet Gynecol. 2021 May 19;2021:9912271. doi: 10.1155/2021/9912271. eCollection 2021. Case Rep Obstet Gynecol. 2021. PMID: 34104501 Free PMC article.
-
The Impact of Uterus Didelphys on Fertility and Pregnancy.Int J Environ Res Public Health. 2022 Aug 25;19(17):10571. doi: 10.3390/ijerph191710571. Int J Environ Res Public Health. 2022. PMID: 36078286 Free PMC article.
-
Uterus didelphys: two pregnancies, two term breech caesarean deliveries.BMJ Case Rep. 2018 Apr 18;2018:bcr2017221815. doi: 10.1136/bcr-2017-221815. BMJ Case Rep. 2018. PMID: 29669764 Free PMC article.
-
Bladder duplication in the male cat: the first case report in China.BMC Vet Res. 2024 Sep 6;20(1):397. doi: 10.1186/s12917-024-04178-6. BMC Vet Res. 2024. PMID: 39242498 Free PMC article.
-
Successful external cephalic version in a patient with uterus didelphys and fetal malpresentation.BMJ Case Rep. 2019 Nov 19;12(11):e230965. doi: 10.1136/bcr-2019-230965. BMJ Case Rep. 2019. PMID: 31748355 Free PMC article.
References
-
- American Fertility Society. The American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, müllerian anomalies and intrauterine adhesions. Fertil Steril 1988;49:944–55. - PubMed
-
- DeUgarte CM. Embryology of the urogenital system and congenital anomalies of the genital tract : DeCherney AH, Nathan L, Lauger N et al., Current diagnosis and treatment: obstetrics and gynecology. New York: Mcgraw-Hill, 2013:38–66.
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources