

Perinatal and maternal morbidity and mortality after attempted operative vaginal delivery at midpelvic station
- PMID: 28584040
- PMCID: PMC5461125
- DOI: 10.1503/cmaj.161156
Perinatal and maternal morbidity and mortality after attempted operative vaginal delivery at midpelvic station
Abstract
Background: Increased use of operative vaginal delivery (i.e., forceps or vacuum application), of which 20% occurs at midpelvic station, has been advocated to reduce the rate of cesarean delivery. We aimed to quantify severe perinatal and maternal morbidity and mortality associated with attempted midpelvic operative vaginal delivery.
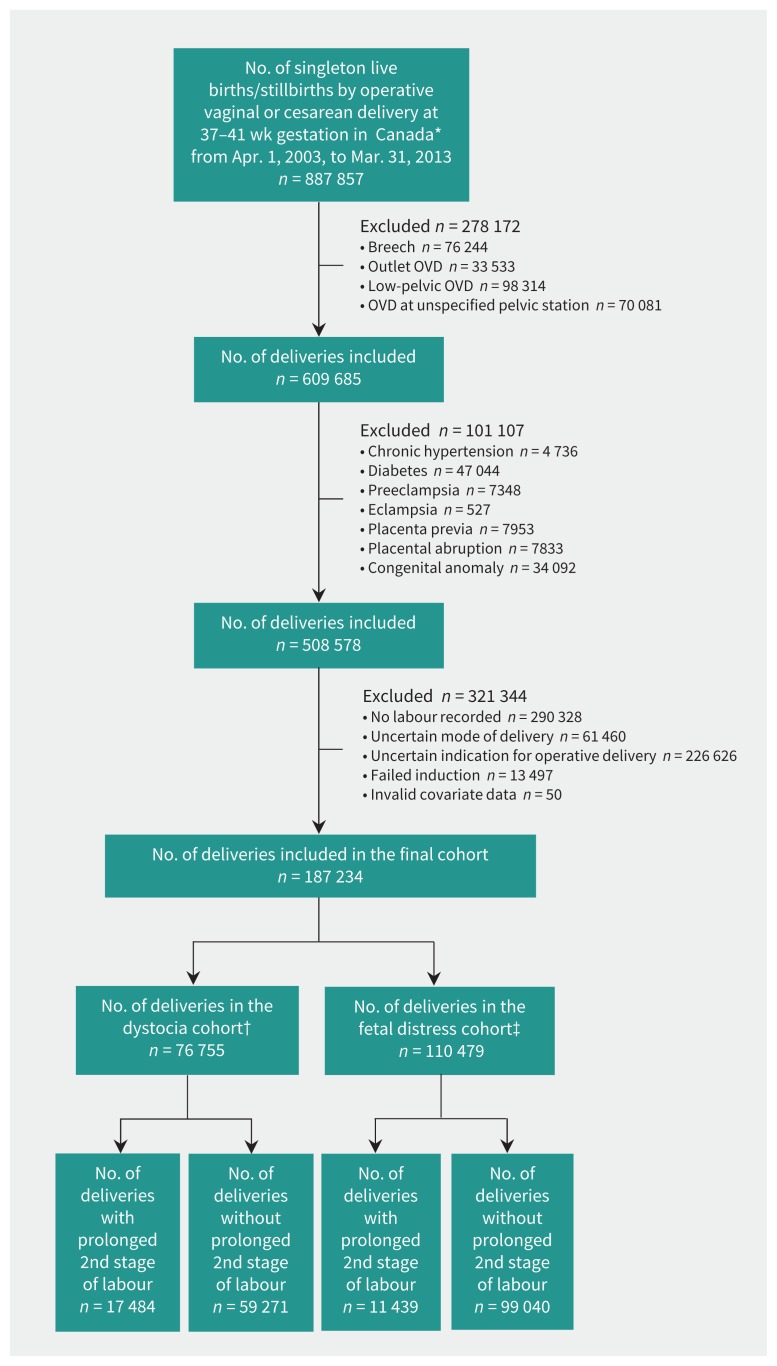
Methods: We studied all term singleton deliveries in Canada between 2003 and 2013, by attempted midpelvic operative vaginal or cesarean delivery with labour (with and without prolonged second stage). The primary outcomes were composite severe perinatal morbidity and mortality (e.g., convulsions, assisted ventilation, severe birth trauma and perinatal death), and composite severe maternal morbidity and mortality (e.g., severe postpartum hemorrhage, shock, sepsis, cardiac complications, acute renal failure and death).
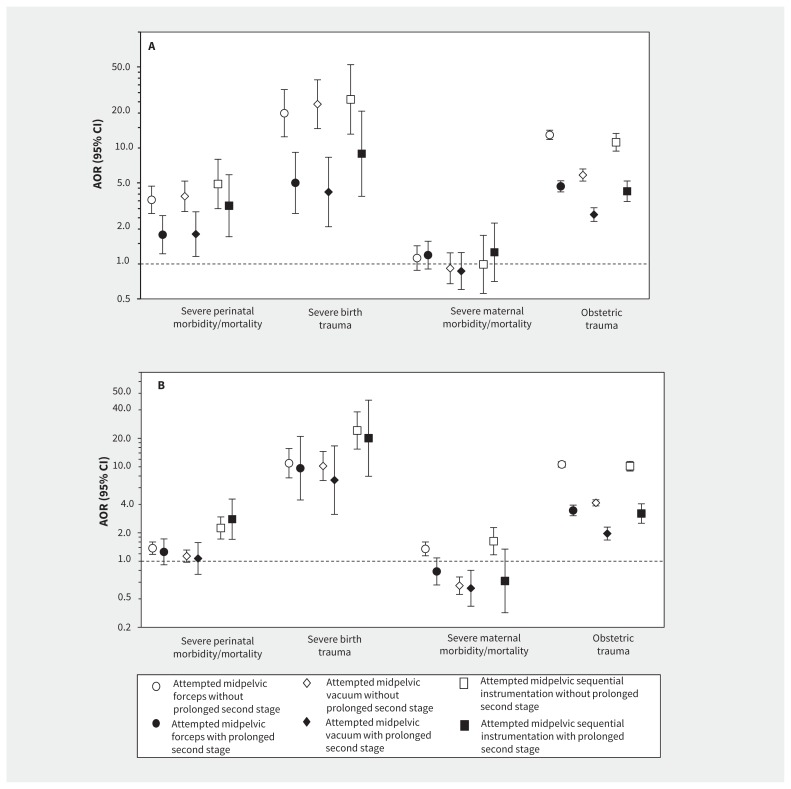
Results: The study population included 187 234 deliveries. Among women with dystocia and prolonged second stage of labour, midpelvic operative vaginal delivery was associated with higher rates of severe perinatal morbidity and mortality compared with cesarean delivery (forceps, adjusted odds ratio [AOR] 1.81, 95% confidence interval [CI] 1.24 to 2.64; vacuum, AOR 1.81, 95% CI 1.17 to 2.80; sequential instruments, AOR 3.19, 95% CI 1.73 to 5.88), especially with higher rates of severe birth trauma. Rates of severe maternal morbidity and mortality were not significantly different after operative vaginal delivery, although rates of obstetric trauma were higher (forceps, AOR 4.51, 95% CI 4.04 to 5.02; vacuum, AOR 2.70, 95% CI 2.35 to 3.09; sequential instruments, AOR 4.24, 95% CI 3.46 to 5.19). Among women with fetal distress, similar associations were seen for severe birth trauma and obstetric trauma, although vacuum was associated with lower rates of severe maternal morbidity and mortality (AOR 0.52, 95% CI 0.33 to 0.80). Associations tended to be stronger among women without a prolonged second stage.
Interpretation: Midpelvic operative vaginal delivery is associated with higher rates of severe birth trauma and obstetric trauma, whereas overall rates of severe perinatal and maternal morbidity and mortality vary by indication and operative instrument.
© 2017 Canadian Medical Association or its licensors.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Beware selection bias.CMAJ. 2017 Aug 28;189(34):E1096. doi: 10.1503/cmaj.733261. CMAJ. 2017. PMID: 28847782 Free PMC article. No abstract available.
-
The end of forceps deliveries?CMAJ. 2017 Aug 28;189(34):E1097. doi: 10.1503/cmaj.733247. CMAJ. 2017. PMID: 28847783 Free PMC article. No abstract available.
-
The authors reply to "The end of forceps deliveries?" and "Beware selection bias".CMAJ. 2017 Aug 28;189(34):E1098. doi: 10.1503/cmaj.733285. CMAJ. 2017. PMID: 28847784 Free PMC article. No abstract available.
-
Data limitations may affect conclusions in study of vaginal delivery at midpelvic station.CMAJ. 2017 Oct 30;189(43):E1343. doi: 10.1503/cmaj.733316. CMAJ. 2017. PMID: 29084762 Free PMC article. No abstract available.
-
Response to "Data limitations may affect conclusions in study of vaginal delivery at midpelvic station".CMAJ. 2017 Oct 30;189(43):E1344-E1345. doi: 10.1503/cmaj.733350. CMAJ. 2017. PMID: 29084763 Free PMC article. No abstract available.
References
-
- Cunningham FG, Leveno KJ, Bloom SL, et al., editors. Operative vaginal delivery. In: Williams obstetrics. 24th ed. New York: McGraw-Hill Education; 2014.
-
- American College of Obstetricians and Gynecologists. Practice Bulletin No. 154: Operative vaginal delivery. Obstet Gynecol 2015;126:e56–65. - PubMed
-
- Alexander JM, Leveno KJ, Hauth J, et al. Fetal injury associated with cesarean delivery. Obstet Gynecol 2006;108:885–90. - PubMed
-
- Alexander JM, Leveno KJ, Rouse DJ, et al. Comparison of maternal and infant outcomes from primary cesarean delivery during the second compared with first stage of labor. Obstet Gynecol 2007;109:917–21. - PubMed
-
- Caughey AB, Cahill AG, Guise JM, et al. Safe prevention of the primary cesarean delivery. Am J Obstet Gynecol 2014;210:179–93. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical