

Advanced Diagnostic Techniques in Autoimmune Bullous Diseases
- PMID: 28584369
- PMCID: PMC5448261
- DOI: 10.4103/ijd.IJD_196_17
Advanced Diagnostic Techniques in Autoimmune Bullous Diseases
Abstract
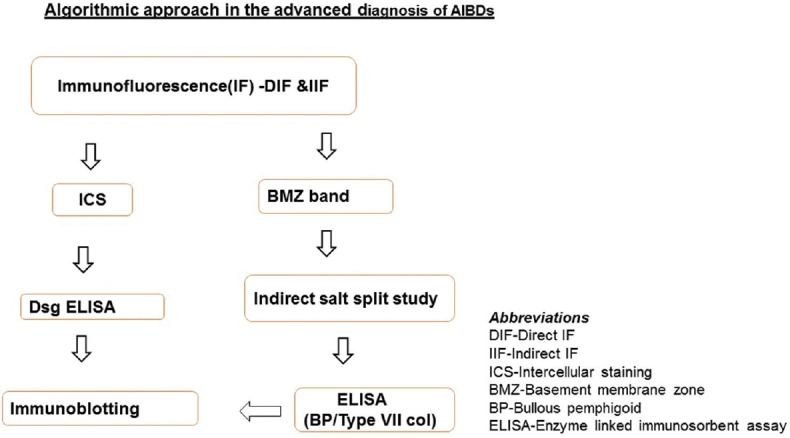
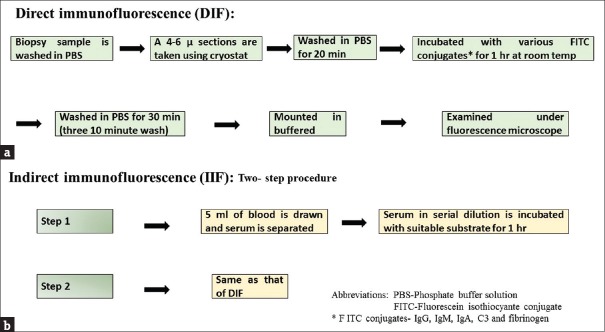
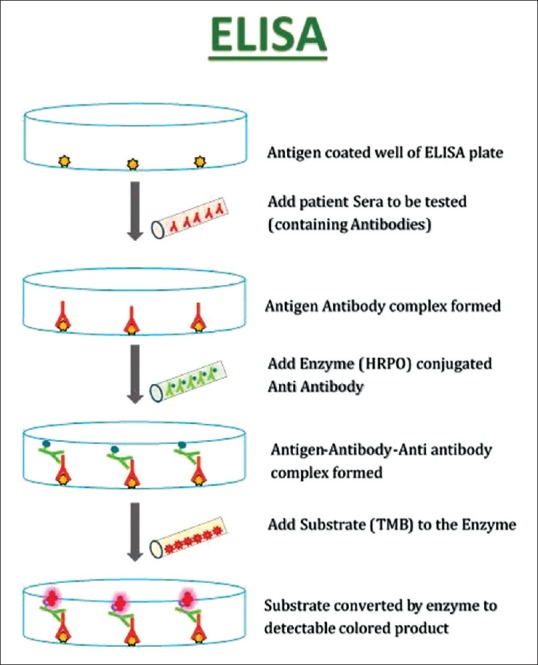
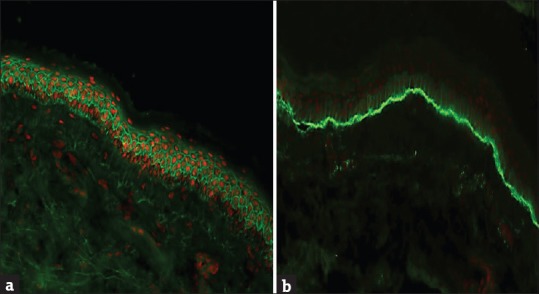
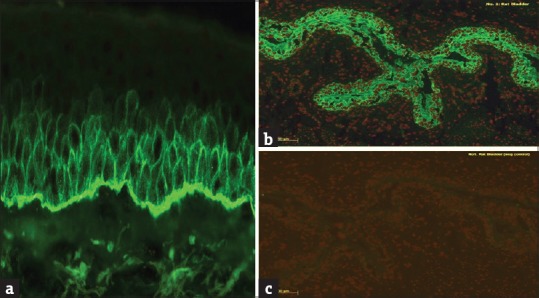
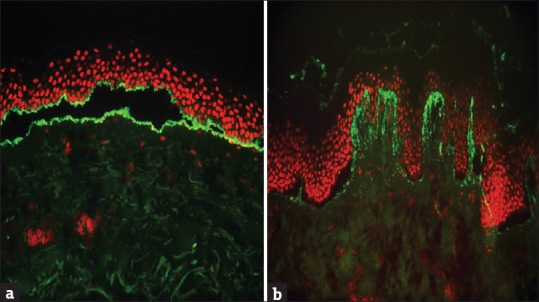
Autoimmune blistering diseases are diverse group of conditions characterized by blisters in the skin with or without mucosal lesions. There may be great degree of clinical and histopathological overlap; hence, advanced immunological tests may be necessary for more precise diagnosis of these conditions. Direct immunofluorescence microscopy is the gold standard tests to demonstrate the tissue-bound antibodies and should be done in all cases. Magnitude of antibody level in patient' serum can be assessed by indirect immunofluorescence and enzyme linked immunosorbent assay. In this article we have reviewed the various techniques that are available in the diagnosis of autoimmune blistering diseases.
Keywords: Autoimmune bullous diseases; ELISA; direct immunofluorescence.
Conflict of interest statement
There are no conflicts of interest. What is new? Honey may be used as an alternate transport medium of skin biopsy specimen for immunofluorescence studiesWhenever possible diagnosis of autoimmune blistering disease should be confirmed by advanced immunological tests.
Figures

Similar articles
-
Enzyme-linked immunosorbent assay in autoimmune blistering diseases: preliminary experience of the Dermatology Department of Cagliari.G Ital Dermatol Venereol. 2008 Feb;143(1):1-8. G Ital Dermatol Venereol. 2008. PMID: 18833046 Clinical Trial.
-
Diagnosis of autoimmune bullous skin diseases.Clin Lab. 2008;54(11-12):491-503. Clin Lab. 2008. PMID: 19216255 Review.
-
Autoimmune bullous skin diseases. Part 2: diagnosis and therapy.J Dtsch Dermatol Ges. 2011 Nov;9(11):927-47. doi: 10.1111/j.1610-0387.2011.07809.x. J Dtsch Dermatol Ges. 2011. PMID: 22026362 Review. English, German.
-
Epidermolysis bullosa acquisita and anti-p200 pemphigoid as major subepidermal autoimmune bullous diseases diagnosed by floor binding on indirect immunofluorescence microscopy using human salt-split skin.Indian J Dermatol Venereol Leprol. 2017 Sep-Oct;83(5):550-555. doi: 10.4103/ijdvl.IJDVL_678_16. Indian J Dermatol Venereol Leprol. 2017. PMID: 28749386
-
Evaluation of clinical and histopathologic/direct immunofluorescence diagnosis in autoimmune vesiculobullous dermatitis: utility of direct immunofluorescence.Turk Patoloji Derg. 2012;28(1):11-6. doi: 10.5146/tjpath.2012.01091. Turk Patoloji Derg. 2012. PMID: 22207426
Cited by
-
Diagnostic Techniques in Autoimmune Blistering Diseases.Br J Biomed Sci. 2023 Nov 24;80:11809. doi: 10.3389/bjbs.2023.11809. eCollection 2023. Br J Biomed Sci. 2023. PMID: 38074463 Free PMC article. Review.
-
Bullous Pemphigoid and Other Pemphigoid Dermatoses.Medicina (Kaunas). 2021 Oct 4;57(10):1061. doi: 10.3390/medicina57101061. Medicina (Kaunas). 2021. PMID: 34684098 Free PMC article. Review.
-
Diagnostic Utility of Direct Immunofluorescence on Paraffin-Embedded Skin Biopsy Samples for the Diagnosis of Autoimmune Vesiculobullous Lesions.Cureus. 2024 Mar 25;16(3):e56916. doi: 10.7759/cureus.56916. eCollection 2024 Mar. Cureus. 2024. PMID: 38665766 Free PMC article.
-
A Multimodal Approach to Diagnosis of Immunobullous Diseases: Integrating Clinical, Histopathological, and Immunofluorescence Findings.Cureus. 2025 May 22;17(5):e84634. doi: 10.7759/cureus.84634. eCollection 2025 May. Cureus. 2025. PMID: 40546482 Free PMC article.
-
Conceptualization and validation of an innovative direct immunofluorescence technique utilizing fluorescein conjugate against IgG + IgG4 for routinely diagnosing autoimmune bullous dermatoses.Cent Eur J Immunol. 2021;46(2):183-190. doi: 10.5114/ceji.2021.107028. Epub 2021 Jun 15. Cent Eur J Immunol. 2021. PMID: 34764786 Free PMC article.
References
-
- Stanley JR. Cell adhesion molecules as targets of autoantibodies in pemphigus and pemphigoid, bullous diseases due to defective epidermal cell adhesion. Adv Immunol. 1993;53:291–325. - PubMed
-
- Mutasim DF, Adams BB. Immunofluorescence in dermatology. J Am Acad Dermatol. 2001;45:803–22. - PubMed
-
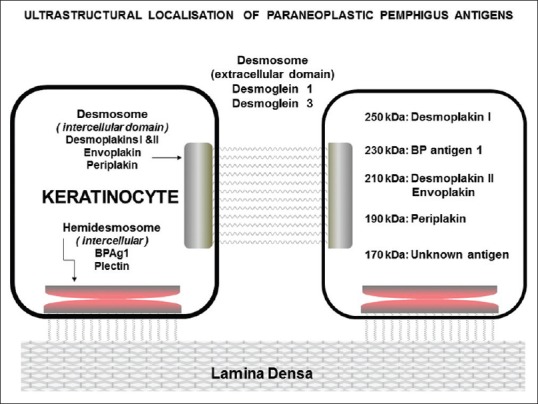
- Anhalt GJ, Kim SC, Stanley JR, Korman NJ, Jabs DA, Kory M, et al. Paraneoplastic pemphigus. An autoimmune mucocutaneous disease associated with neoplasia. N Engl J Med. 1990;323:1729–35. - PubMed
LinkOut - more resources
Full Text Sources