

Serum fatty acid profile in psoriasis and its comorbidity
- PMID: 28585093
- PMCID: PMC5486566
- DOI: 10.1007/s00403-017-1748-x
Serum fatty acid profile in psoriasis and its comorbidity
Abstract
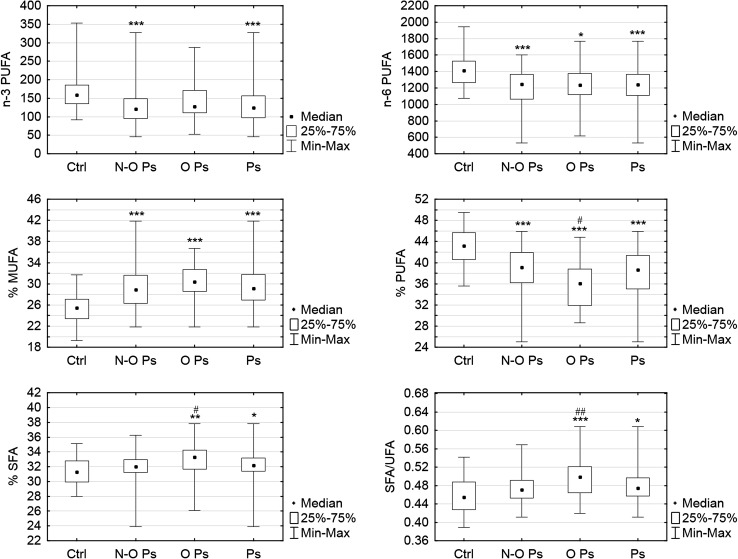
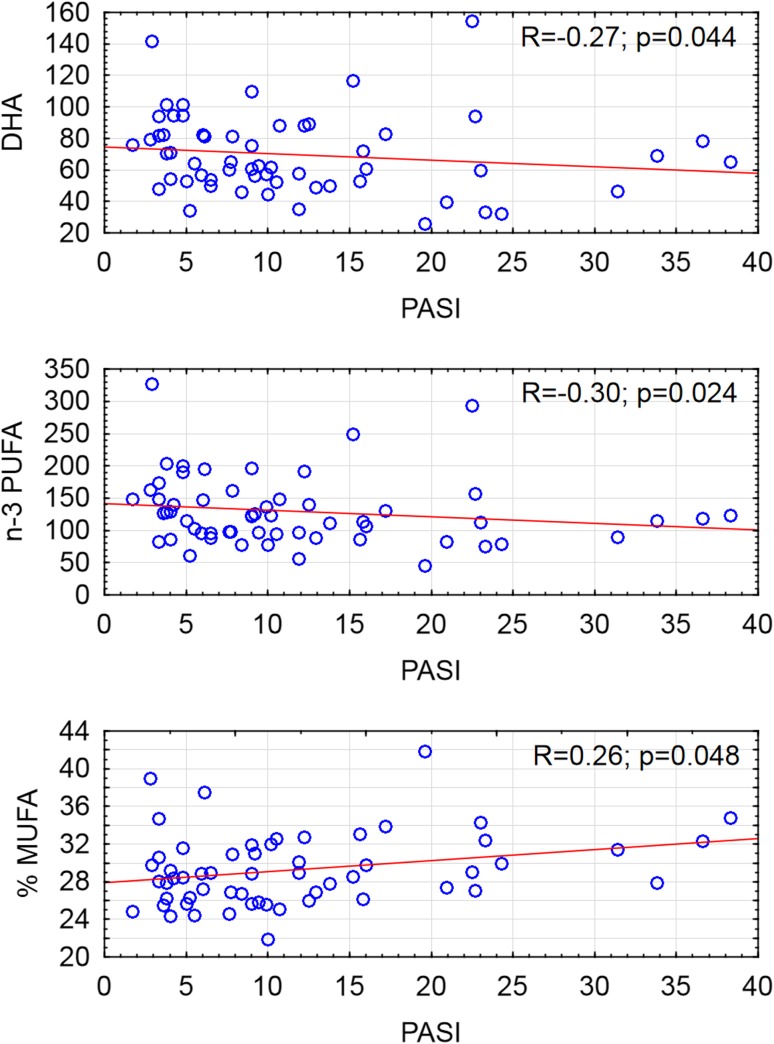
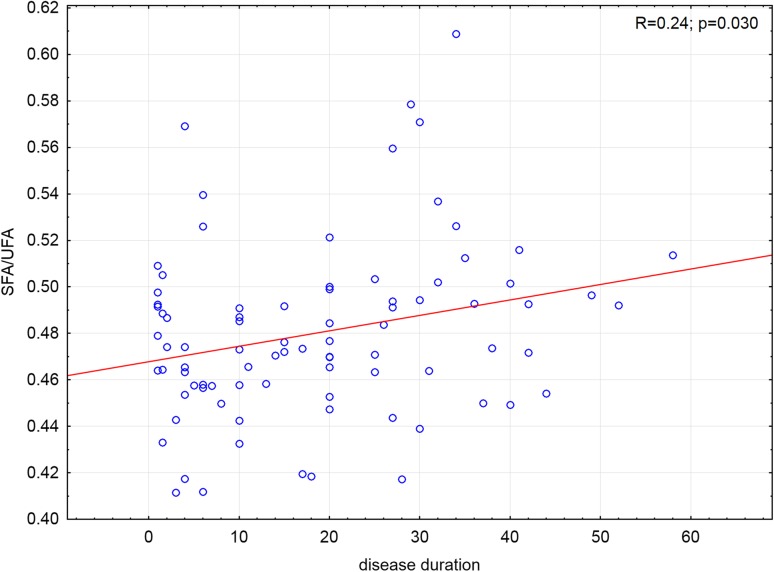
Psoriasis is a chronic inflammatory skin disease that is accompanied by metabolic disturbances and cardio-metabolic disorders. Fatty acids (FAs) might be a link between psoriasis and its comorbidity. The aim of the study was to evaluate serum concentrations of FAs and to investigate their association with the disease activity, markers of inflammation and possible involvement in psoriatic comorbidity: obesity, type 2 diabetes and hypertension. We measured 14 total serum fatty acids content and composition by gas-liquid chromatography and flame-ionization detector after direct in situ transesterification in 85 patients with exacerbated plaque psoriasis and in 32 healthy controls. FAs were grouped according to their biologic properties to saturated FA (SFA), unsaturated FA (UFA), monounsaturated FA (MUFA), n-3 polyunsaturated FA (n-3 PUFA) and n-6 PUFA. Generally, patients characteristic included: Psoriasis Area and Severity Index (PASI), Body Mass Index, inflammatory and biochemical markers, lipid profile and presence of psoriatic comorbidity. We have observed highly abnormal FAs pattern in psoriatic patients both with and without obesity compared to the control group. We have demonstrated association of PASI with low levels of circulating DHA, n-3 PUFA (p = 0.044 and p = 0.048, respectively) and high percent of MUFA (p = 0.024) in the non-obese psoriatic group. The SFA/UFA ratio increased with the duration of the disease (p = 0.03) in all psoriatic patients. These findings indicate abnormal FAs profile in psoriasis which may reflect metabolic disturbances and might play a role in the psoriatic comorbidity.
Keywords: Fatty acid; MUFA; Metabolic syndrome; PUFA; Psoriasis; SFA.
Conflict of interest statement
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
This study was supported by a study grant from the Medical University of Białystok (Project No: N/ST/ZB/16/001/1149).
Ethical approval
All procedures performed in the study involving human participants were in accordance with the ethical standards of the Bioethical Committee of Medical University of Białystok and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Figures
References
-
- Ahlehoff O, Gislason GH, Charlot M, Jorgensen CH, Lindhardsen J, Olesen JB, Abildstrom SZ, Skov L, Torp-Pedersen C, Hansen PR. Psoriasis is associated with clinically significant cardiovascular risk: a Danish nationwide cohort study. J Intern Med. 2011;270:147–157. doi: 10.1111/j.1365-2796.2010.02310.x. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
