

Electrosensitization Increases Antitumor Effectiveness of Nanosecond Pulsed Electric Fields In Vivo
- PMID: 28585492
- PMCID: PMC5762058
- DOI: 10.1177/1533034617712397
Electrosensitization Increases Antitumor Effectiveness of Nanosecond Pulsed Electric Fields In Vivo
Abstract
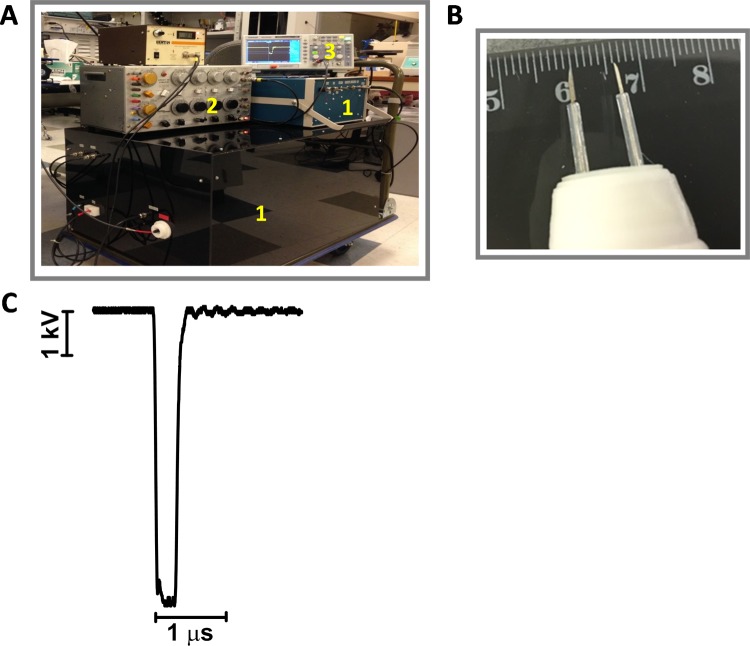
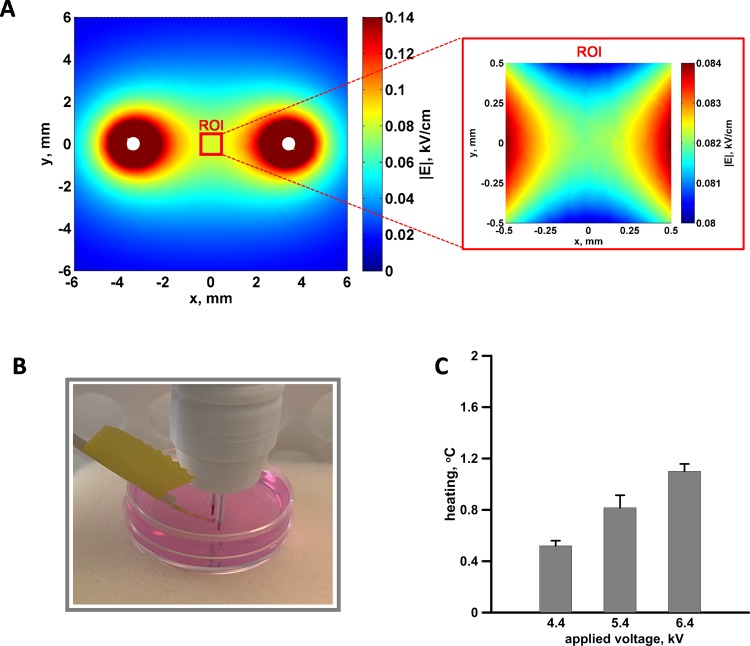
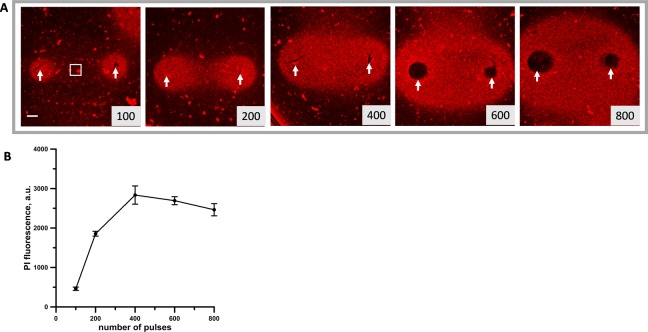
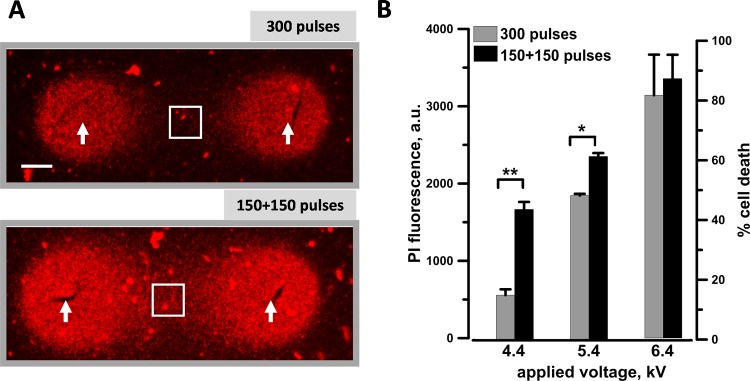
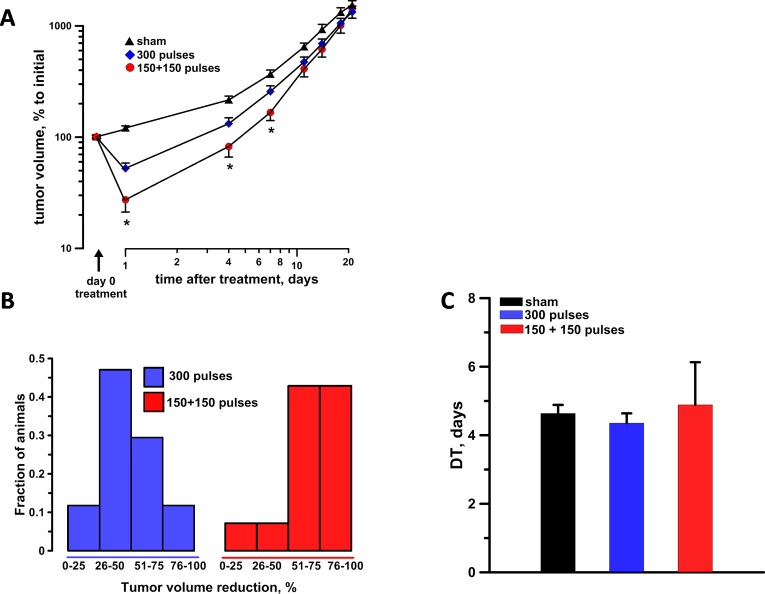
Nanosecond pulsed electric fields are emerging as a new modality for tissue and tumor ablation. We previously reported that cells exposed to pulsed electric fields develop hypersensitivity to subsequent pulsed electric field applications. This phenomenon, named electrosensitization, is evoked by splitting the pulsed electric field treatment in fractions (split-dose treatments) and causes in vitro a 2- to 3-fold increase in cytotoxicity. The aim of this study was to show the benefit of split-dose treatments for in vivo tumor ablation by nanosecond pulsed electric field. KLN 205 squamous carcinoma cells were embedded in an agarose gel or grown subcutaneously as tumors in mice. Nanosecond pulsed electric field ablations were produced using a 2-needle probe with a 6.5-mm interelectrode distance. In agarose gel, splitting a pulsed electric field dose of 300, 300-ns pulses (20 Hz, 4.4-6.4 kV) in 2 equal fractions increased cell death up to 3-fold compared to single-train treatments. We then compared the antitumor effectiveness of these treatments in vivo. At 24 hours after treatment, sensitizing tumors by a split-dose pulsed electric field exposure (150 + 150, 300-ns pulses, 20 Hz, 6.4 kV) caused a 4- and 2-fold tumor volume reduction as compared to sham and single-train treatments, respectively. Tumor volume reduction that exceeds 75% was 43% for split-dose-treated animals compared to only 12% for single-dose treatments. The difference between the 2 experimental groups remained statistically significant for at least 1 week after the treatment. The results show that electrosensitization occurs in vivo and can be exploited to assist in vivo cancer ablation.
Keywords: electrosensitization; irreversible electroporation; nanoporation; nanosecond pulsed electric fields (nsPEF); tumor ablation.
Conflict of interest statement
Figures
References
-
- Jiang C, Davalos RV, Bischof JC. A review of basic to clinical studies of irreversible electroporation therapy. IEEE Trans Biomed Eng. 2015;62(1):4–20. - PubMed
-
- Rubinsky B. Irreversible electroporation in medicine. Technol Cancer Res Treat. 2007;6(4):255–260. - PubMed
-
- Bhonsle S, Bonakdar M, Neal RE, II, et al. Characterization of irreversible electroporation ablation with a validated perfused organ model. J Vasc Interv Radiol. 2016;27(12):1913–1922.e2. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
