

Fecal microbiota transplant from a rational stool donor improves hepatic encephalopathy: A randomized clinical trial
- PMID: 28586116
- PMCID: PMC6102730
- DOI: 10.1002/hep.29306
Fecal microbiota transplant from a rational stool donor improves hepatic encephalopathy: A randomized clinical trial
Abstract
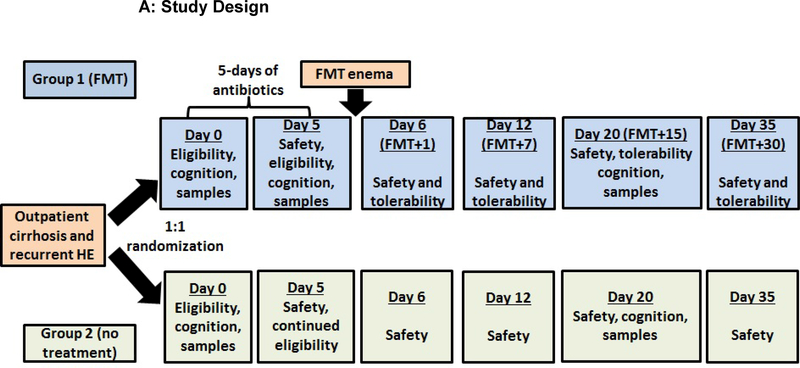
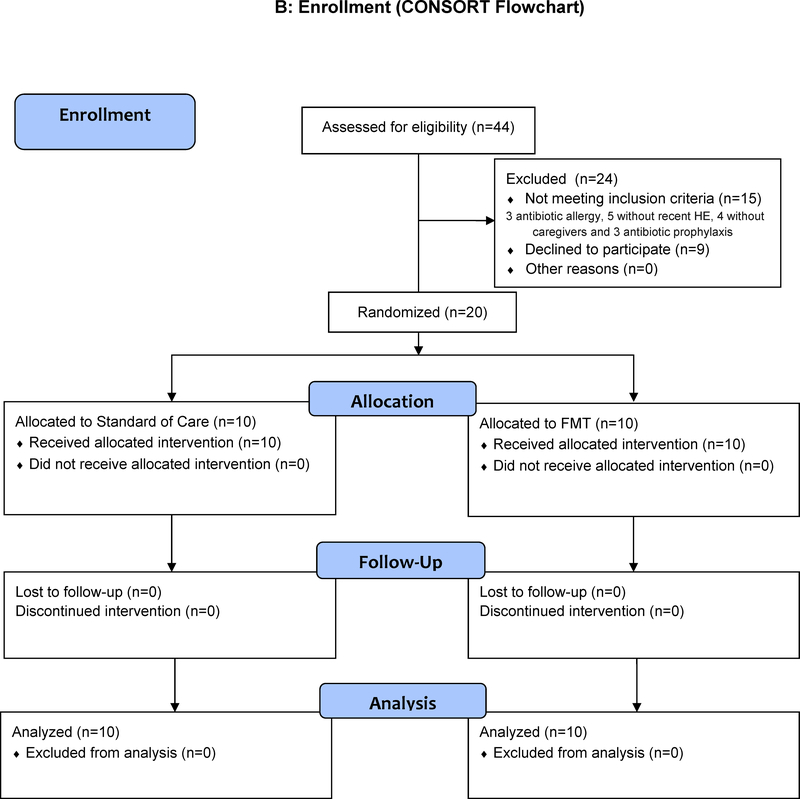
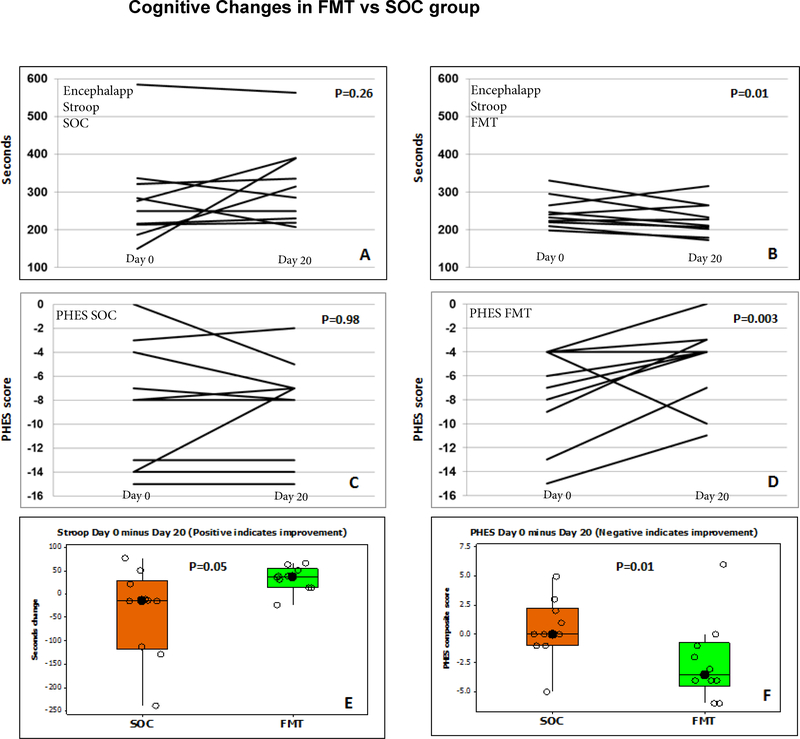
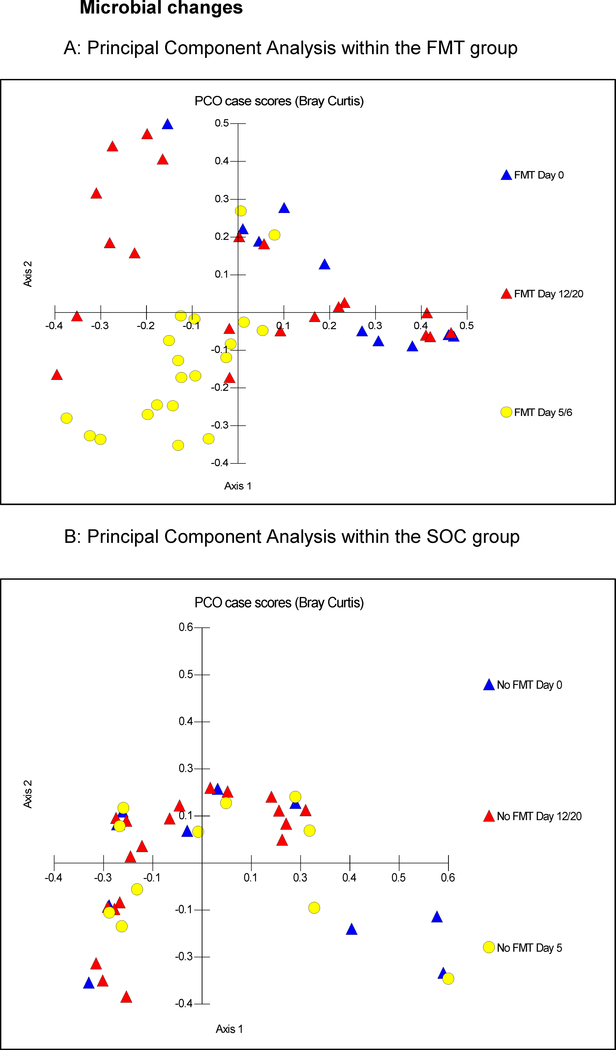
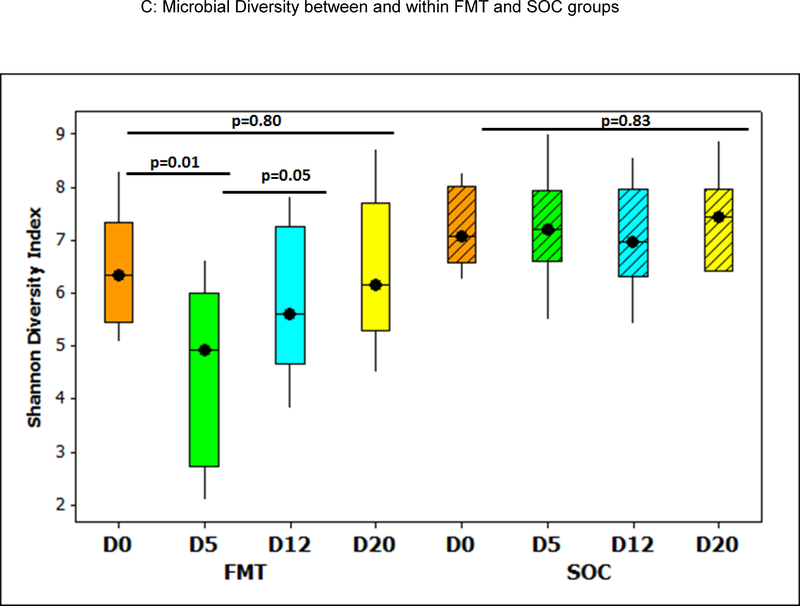
Recurrent hepatic encephalopathy (HE) is a leading cause of readmission despite standard of care (SOC) associated with microbial dysbiosis. Fecal microbiota transplantation (FMT) may improve dysbiosis; however, it has not been studied in HE. We aimed to define whether FMT using a rationally derived stool donor is safe in recurrent HE compared to SOC alone. An open-label, randomized clinical trial with a 5-month follow-up in outpatient men with cirrhosis with recurrent HE on SOC was conducted with 1:1 randomization. FMT-randomized patients received 5 days of broad-spectrum antibiotic pretreatment, then a single FMT enema from the same donor with the optimal microbiota deficient in HE. Follow-up occurred on days 5, 6, 12, 35, and 150 postrandomization. The primary outcome was safety of FMT compared to SOC using FMT-related serious adverse events (SAEs). Secondary outcomes were adverse events, cognition, microbiota, and metabolomic changes. Participants in both arms were similar on all baseline criteria and were followed until study end. FMT with antibiotic pretreatment was well tolerated. Eight (80%) SOC participants had a total of 11 SAEs compared to 2 (20%) FMT participants with SAEs (both FMT unrelated; P = 0.02). Five SOC and no FMT participants developed further HE (P = 0.03). Cognition improved in the FMT, but not the SOC, group. Model for End-Stage Liver Disease (MELD) score transiently worsened postantibiotics, but reverted to baseline post-FMT. Postantibiotics, beneficial taxa, and microbial diversity reduction occurred with Proteobacteria expansion. However, FMT increased diversity and beneficial taxa. SOC microbiota and MELD score remained similar throughout.
Conclusion: FMT from a rationally selected donor reduced hospitalizations, improved cognition, and dysbiosis in cirrhosis with recurrent HE. (Hepatology 2017;66:1727-1738).
© 2017 by the American Association for the Study of Liver Diseases.
Figures
Comment in
-
Fecal microbiota transplant from a rational stool donor improves hepatic encephalopathy: A randomized clinical trial.Hepatology. 2017 Oct;66(4):1354-1355. doi: 10.1002/hep.29369. Epub 2017 Aug 26. Hepatology. 2017. PMID: 28714089 No abstract available.
-
Reply.Hepatology. 2017 Oct;66(4):1355-1356. doi: 10.1002/hep.29368. Epub 2017 Aug 26. Hepatology. 2017. PMID: 28714102 No abstract available.
-
Fecal microbiota transplantation for hepatic encephalopathy: Ready for prime time?Hepatology. 2017 Dec;66(6):1713-1715. doi: 10.1002/hep.29396. Epub 2017 Oct 30. Hepatology. 2017. PMID: 28734127 No abstract available.
-
Fecal microbiota transplantation for treating recurrent hepatic encephalopathy: Ready for clinical application?Turk J Gastroenterol. 2017 Sep;28(5):425-426. doi: 10.5152/tjg.2017.18817. Turk J Gastroenterol. 2017. PMID: 28936973 No abstract available.
References
-
- Vilstrup H, Amodio P, Bajaj J, Cordoba J, Ferenci P, Mullen KD, Weissenborn K, et al. Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver. Hepatology 2014;60:715–735. - PubMed
-
- Stepanova M, Mishra A, Venkatesan C, Younossi ZM. In-hospital mortality and economic burden associated with hepatic encephalopathy in the United States from 2005 to 2009. Clin Gastroenterol Hepatol 2012;10:1034–1041 e1031. - PubMed
-
- Fernandez J, Tandon P, Mensa J, Garcia-Tsao G. Antibiotic prophylaxis in cirrhosis: Good and bad. Hepatology 2016;63:2019–2031. - PubMed
-
- Bajaj JS, O’Leary JG, Reddy KR, Wong F, Olson JC, Subramanian RM, Brown G, et al. Second infections independently increase mortality in hospitalized patients with cirrhosis: the North American consortium for the study of end-stage liver disease (NACSELD) experience. Hepatology 2012;56:2328–2335. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
