

Improved posttransplant mortality after share 35 for liver transplantation
- PMID: 28586179
- PMCID: PMC5756050
- DOI: 10.1002/hep.29301
Improved posttransplant mortality after share 35 for liver transplantation
Abstract
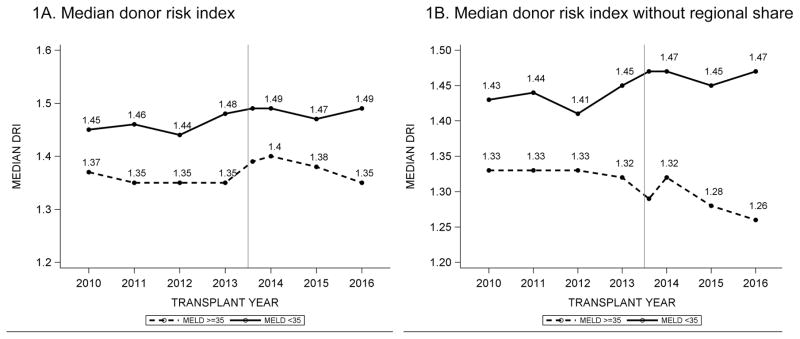
The Share 35 policy was implemented in June 2013 to improve equity in access to liver transplantation (LT) between patients with fulminant liver failure and those with cirrhosis and severe hepatic decompensation. The aim of this study was to assess post-LT outcomes after Share 35. Relevant donor, procurement, and recipient data were extracted from the Organ Procurement and Transplantation Network/United Network for Organ Sharing database. All adult deceased donor LTs from January 1, 2010, to March 31, 2016, were included in the analysis. One-year patient survival before and after Share 35 was assessed by multivariable Cox proportional hazards analysis, with adjustment for variables known to affect graft survival. Of 34,975 adult LT recipients, 16,472 (47.1%) were transplanted after the implementation of Share 35, of whom 4,599 (27.9%) had a Model for End-Stage Liver Disease (MELD) score ≥35. One-year patient survival improved from 83.9% to 88.4% after Share 35 (P < 0.01) for patients with MELD ≥35. There was no significant impact on survival of patients with MELD <35 (P = 0.69). Quality of donor organs, as measured by a donor risk index without the regional share component, improved for patients with MELD ≥35 (P < 0.01) and worsened for patients with lower MELD (P < 0.01). In multivariable Cox regression analysis, Share 35 was associated with improved 1-year patient survival (hazard ratio, 0.69; 95% confidence interval, 0.60-0.80) in recipients with MELD ≥35.
Conclusion: Share 35 has had a positive impact on survival after transplantation in patients with MELD ≥35, without a reciprocal detriment in patients with lower acuity; this was in part a result of more favorable donor-recipient matching. (Hepatology 2018;67:273-281).
© 2017 by the American Association for the Study of Liver Diseases.
Conflict of interest statement
Figures

Comment in
-
The benefit of sharing.Hepatology. 2018 Jan;67(1):16-17. doi: 10.1002/hep.29467. Epub 2017 Nov 29. Hepatology. 2018. PMID: 28806474 No abstract available.
References
-
- Kamath PS, Wiesner RH, Malinchoc M, Kremers W, Therneau TM, Kosberg CL, D’Amico G, et al. A model to predict survival in patients with end-stage liver disease. Hepatology. 2001;33:464–470. - PubMed
-
- Freeman RB, Wiesner RH, Edwards E, Harper A, Merion R, Wolfe R UNOS/OPTN Liver and Transplantation Committee. Results of the first year of the new liver allocation plan. Liver Transpl. 2004;10:7–15. - PubMed
-
- Washburn K, Harper A, Klintmalm G, Goss J, Halff G. Regional sharing for adult status 1 candidates: reduction in waitlist mortality. Liver Transpl. 2006;12:470–474. - PubMed
-
- Edwards EB, Harper AM, Hirose R, Mulligan DC. The impact of broader regional sharing of livers: 2-year results of “Share 35”. Liver Transpl. 2016;22:399–409. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
