

Effect of Nebulized Hypertonic Saline Treatment in Emergency Departments on the Hospitalization Rate for Acute Bronchiolitis: A Randomized Clinical Trial
- PMID: 28586918
- PMCID: PMC6583778
- DOI: 10.1001/jamapediatrics.2017.1333
Effect of Nebulized Hypertonic Saline Treatment in Emergency Departments on the Hospitalization Rate for Acute Bronchiolitis: A Randomized Clinical Trial
Abstract
Importance: Acute bronchiolitis is the leading cause of hospitalization among infants. Previous studies, underpowered to examine hospital admission, have found a limited benefit of nebulized hypertonic saline (HS) treatment in the pediatric emergency department (ED).
Objective: To examine whether HS nebulization treatment would decrease the hospital admission rate among infants with a first episode of acute bronchiolitis.
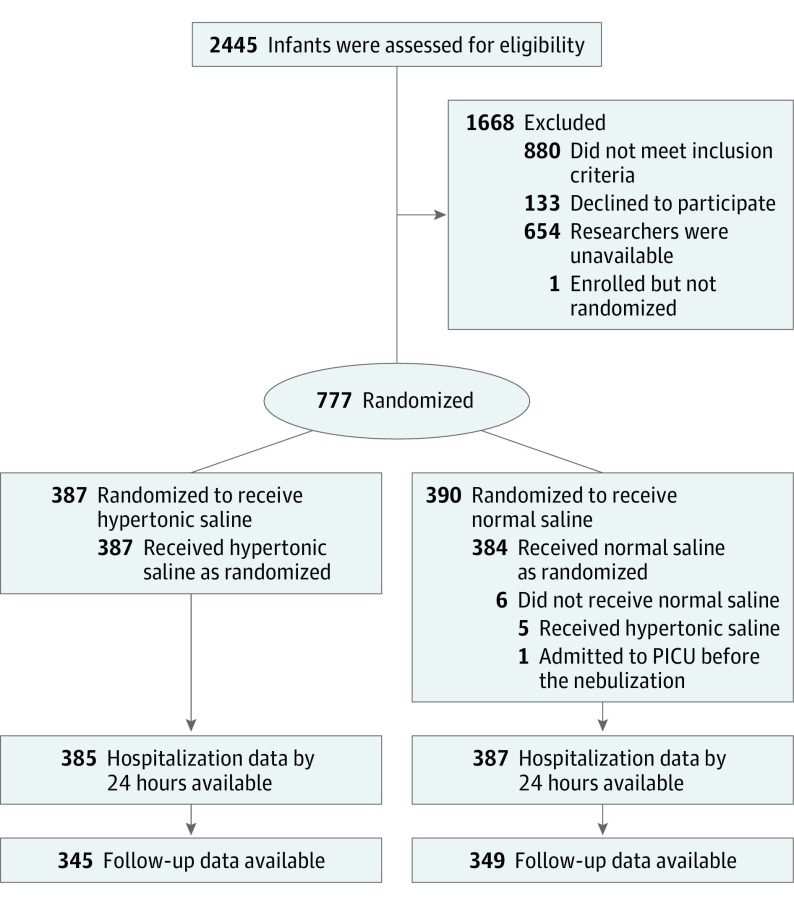
Design, setting, and participants: The Efficacy of 3% Hypertonic Saline in Acute Viral Bronchiolitis (GUERANDE) study was a multicenter, double-blind randomized clinical trial on 2 parallel groups conducted during 2 bronchiolitis seasons (October through March) from October 15, 2012, through April 15, 2014, at 24 French pediatric EDs. Among the 2445 infants (6 weeks to 12 months of age) assessed for inclusion, 777 with a first episode of acute bronchiolitis with respiratory distress and no chronic medical condition were included.
Interventions: Two 20-minute nebulization treatments of 4 mL of HS, 3%, or 4 mL of normal saline (NS), 0.9%, given 20 minutes apart.
Main outcomes and measures: Hospital admission rate in the 24 hours after enrollment.
Results: Of the 777 infants included in the study (median age, 3 months; interquartile range, 2-5 months; 468 [60.2%] male), 385 (49.5%) were randomized to the HS group and 387 (49.8%) to the NS group (5 patients did not receive treatment). By 24 hours, 185 of 385 infants (48.1%) in the HS group were admitted compared with 202 of 387 infants (52.2%) in the NS group. The risk difference for hospitalizations was not significant according to the mixed-effects regression model (adjusted risk difference, -3.2%; 95% CI, -8.7% to 2.2%; P = .25). The mean (SD) Respiratory Distress Assessment Instrument score improvement was greater in the HS group (-3.1 [3.2]) than in the NS group (-2.4 [3.3]) (adjusted difference, -0.7; 95% CI, -1.2 to -0.2; P = .006) and similarly for the Respiratory Assessment Change Score. Mild adverse events, such as worsening of cough, occurred more frequently among children in the HS group (35 of 392 [8.9%]) than among those in the NS group (15 of 384 [3.9%]) (risk difference, 5.0%; 95% CI, 1.6%-8.4%; P = .005), with no serious adverse events.
Conclusions and relevance: Nebulized HS treatment did not significantly reduce the rate of hospital admissions among infants with a first episode of acute moderate to severe bronchiolitis who were admitted to the pediatric ED relative to NS, but mild adverse events were more frequent in the HS group.
Trial registration: clinicaltrials.gov Identifier: NCT01777347.
Conflict of interest statement
Figures
Comment in
-
Hypertonic Saline and Acute Bronchiolitis: The Debate Is Still On.JAMA Pediatr. 2018 Jan 1;172(1):93. doi: 10.1001/jamapediatrics.2017.3805. JAMA Pediatr. 2018. PMID: 29114734 No abstract available.
-
Hypertonic Saline and Acute Bronchiolitis-Reply.JAMA Pediatr. 2018 Jan 1;172(1):93-94. doi: 10.1001/jamapediatrics.2017.3799. JAMA Pediatr. 2018. PMID: 29114843 No abstract available.
References
-
- Johnson LW, Robles J, Hudgins A, Osburn S, Martin D, Thompson A. Management of bronchiolitis in the emergency department: impact of evidence-based guidelines? Pediatrics. 2013;131(suppl 1):S103-S109. - PubMed
-
- Pelletier AJ, Mansbach JM, Camargo CA Jr. Direct medical costs of bronchiolitis hospitalizations in the United States. Pediatrics. 2006;118(6):2418-2423. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
