

Three-dimensional arterial spin labeling imaging and dynamic susceptibility contrast perfusion-weighted imaging value in diagnosing glioma grade prior to surgery
- PMID: 28587332
- PMCID: PMC5450692
- DOI: 10.3892/etm.2017.4370
Three-dimensional arterial spin labeling imaging and dynamic susceptibility contrast perfusion-weighted imaging value in diagnosing glioma grade prior to surgery
Abstract
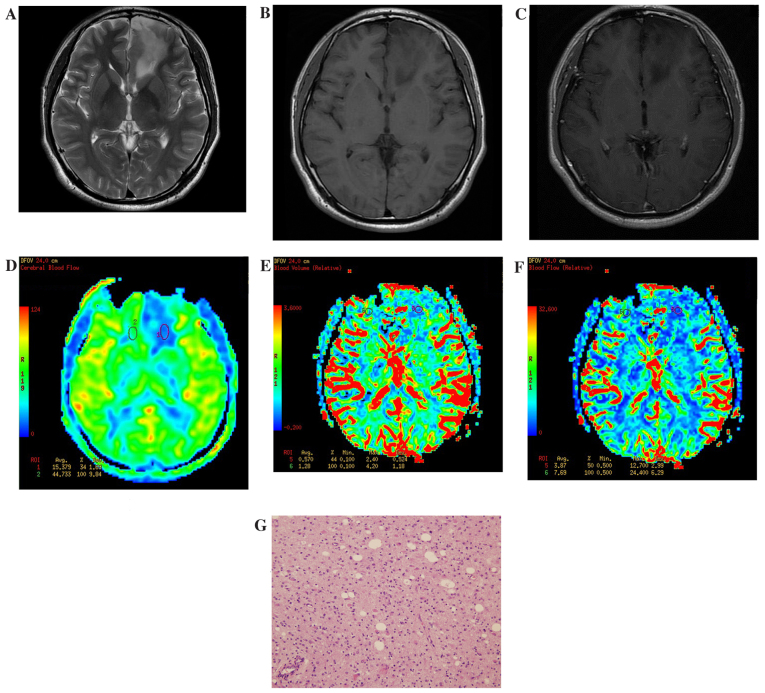
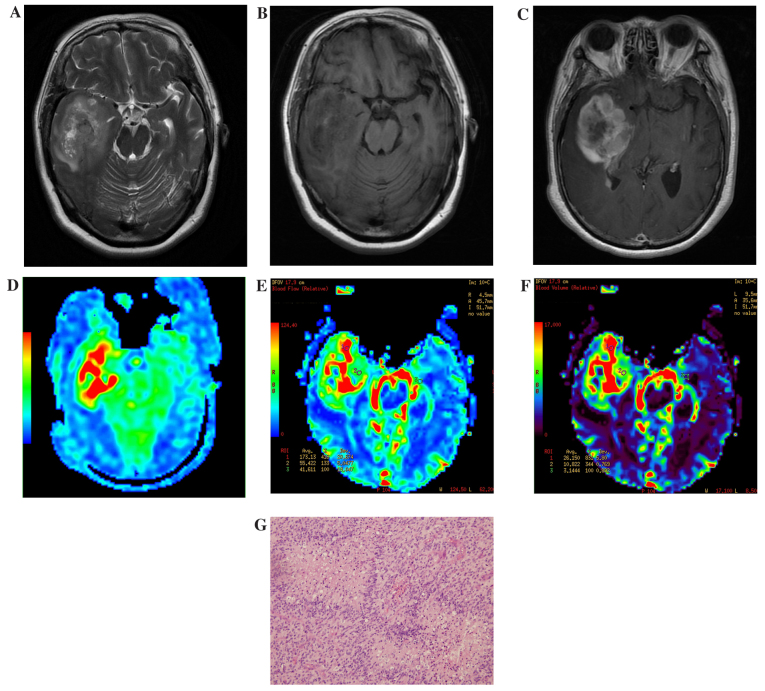
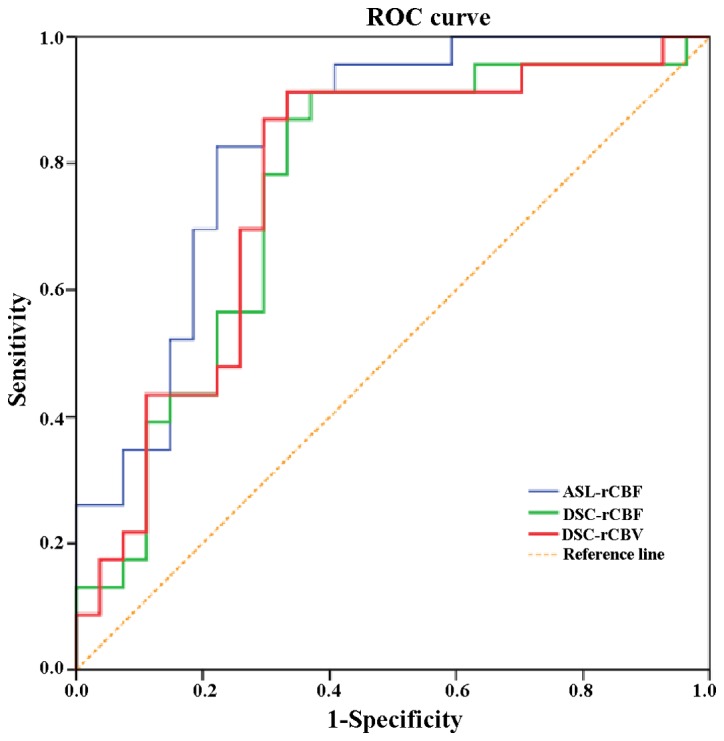
The current study aimed to investigate whole-brain three-dimensional arterial spin labeling imaging (3D ASL) and dynamic susceptibility contrast perfusion-weighted imaging (DSC-PWI), in regards to their diagnostic value of preoperative glioma grade. The parameter values obtained after correction will be correlated with the diagnostic value of 3D ASL and DSC-PWI perfusion. In the current study, 50 patients with gliomas confirmed by pathology were used, including 27 low-grade gliomas (LGGs) and 23 high-grade gliomas (HGGs). Prior to surgery all patients underwent 3 Tesla magnetic resonance imaging (MRI), 3D ASL, DSC-PWI and conventional enhanced MRI scans to obtain original 3D ASL and DSC-PWI images, and the tumor regions with the most obvious parenchyma perfusion and contralateral normal white matter were selected. In these areas, the ASL-relative cerebral blood flow (ASL-rCBF), DSC-relative cerebral blood flow (DSC-rCBF) and DSC-relative cerebral blood volume (DSC-rCBV) parameter values were then obtained after correction for individual differences. The results of the present study show that ASL-CBF, DSC-CBF, DSC-CBV values and ASL-rCBF, DSC-rCBF, DSC-rCBV values increased as the grade of the glioma being imaged increased, and there was a marked difference between the HGGs and the LGGs. ASL-rCBF was significantly positively correlated with DSC-rCBF (r=0.580, P<0.01). In addition, ASL-rCBF was significantly positively correlated with DSC-rCBV (r=0.431, P<0.01). Receiver operating characteristic (ROC) curves were applied to compare the two perfusion parameters of DSC-PWI and 3D ASL in the diagnosis of glioma grade. ASL-rCBF had the highest area value under the ROC curve (0.836). The areas under the ROC curve of DSC-rCBF and DSC-rCBV were analyzed using the Z test, but the difference was not statistically significant. When ASL-rCBF, DSC-rCBF and DSC-rCBV were cutoff at 2.24, 1.85 and 1.68, the sensitivity of HGG diagnosis was 83.2, 91.3 and 91.3%, and the specificity was 77.7, 63.9 and 66.7%, respectively.
Keywords: dynamic susceptibility contrast perfusion-weighted imaging; glioma; magnetic resonance imaging; three-dimensional arterial spin labeling.
Figures
References
-
- Brat DJ, Parisi JE, Kleinschmidt-DeMasters BK, Yachnis AT, Montine TJ, Boyer PJ, Powell SZ, Prayson RA, McLendon RE. Neuropathology Committee, College of American Pathologists: Surgical neuropathology update: A review of changes introduced by the WHO classification of tumours of the central nervous system, 4th edition. Arch Pathol Lab Med. 2008;132:993–1007. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources