

GnRH antagonist for patients with polycystic ovary syndrome undergoing controlled ovarian hyperstimulation for in vitro fertilization and embryo transfer in fresh cycles
- PMID: 28587385
- PMCID: PMC5450517
- DOI: 10.3892/etm.2017.4309
GnRH antagonist for patients with polycystic ovary syndrome undergoing controlled ovarian hyperstimulation for in vitro fertilization and embryo transfer in fresh cycles
Abstract
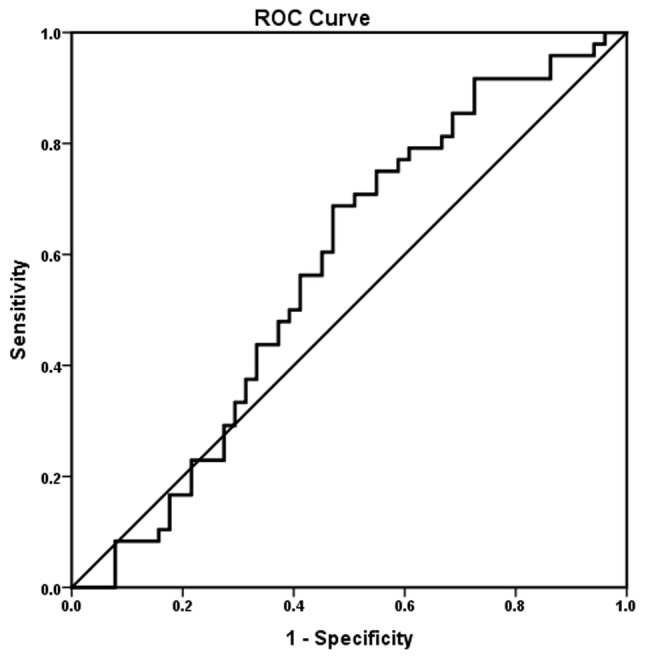
The aim of the present study was to evaluate the influence of a gonadotropin-releasing hormone (GnRH) antagonist compared with a GnRH agonist on the in vitro fertilization cycle outcome in patients with polycystic ovary syndrome. The outcomes of pregnancy were evaluated. The area under the curve (AUC) of the receiver operating characteristic (ROC) curve was also used to evaluate whether the endometrial thickness (cm) and estradiol (E2) level (pg/ml) on the day of human chorionic gonadotropin (hCG) administration (the hCG day) had the best sensitivity and specificity for predicting a clinical pregnancy. The results demonstrated that there were significant differences in the E2 and progesterone levels between the two treatment groups on the hCG day. Furthermore, the mean number of total oocytes retrieved, mean number of 2 pronuclei oocytes, mean number of oocytes cleaved (P<0.05), mean number of embryos available (P=0.022) and mean number of embryos transferred (P=0.014) were significantly different. Additionally, the rates of ectopic pregnancy (P=0.984) and ovarian hyperstimulation syndrome (P=0.976) did not differ significantly between the treatment groups. Although the biochemical pregnancy (P=0.592), clinical pregnancy (P=0.617) and live birth (P=0.365) rates were lower with the GnRH antagonist than with the GnRH agonist, there were no significant differences in the outcomes between the two groups. Analysis of the influence of endometrial thickness with respect to the clinical pregnancy using the ROC (AUC) method revealed that when the best cutoff of 9.75 cm was used, the sensitivity was 62.5%, the specificity was 43.1% and the AUC was 0.53. Additionally, the Youden index was 0.056. Analysis of the influence of the E2 level on the hCG day on clinical pregnancy, using the ROC (AUC) method showed that the best cutoff was 2,984.5 pg/ml, which had a sensitivity of 68.8% and specificity of 52.9%, while the AUC was 0.573 (with a Youden index of 0.217). Furthermore, the results demonstrated that neither the endometrial thickness nor the E2 level on the hCG day had the best sensitivity and specificity for predicting a clinical pregnancy.
Keywords: clinical pregnancy; fresh cycle; gonadotrophin-releasing hormone antagonist; in vitro fertilization and embryo transfer; ovarian hyperstimulation syndrome; polycystic ovary syndrome.
Figures



References
-
- Griesinger G, Diedrich K, Tarlatzis BC, Kolibianakis EM. GnRH-antagonists in ovarian stimulation for IVF in patients with poor response to gonadotrophins, polycystic ovary syndrome and risk of ovarian hyperstimulation: A meta-analysis. Reprod Biomed Online. 2006;13:628–638. doi: 10.1016/S1472-6483(10)60652-9. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources