

MRI features of growth hormone deficiency in children with short stature caused by pituitary lesions
- PMID: 28587427
- PMCID: PMC5450600
- DOI: 10.3892/etm.2017.4377
MRI features of growth hormone deficiency in children with short stature caused by pituitary lesions
Abstract
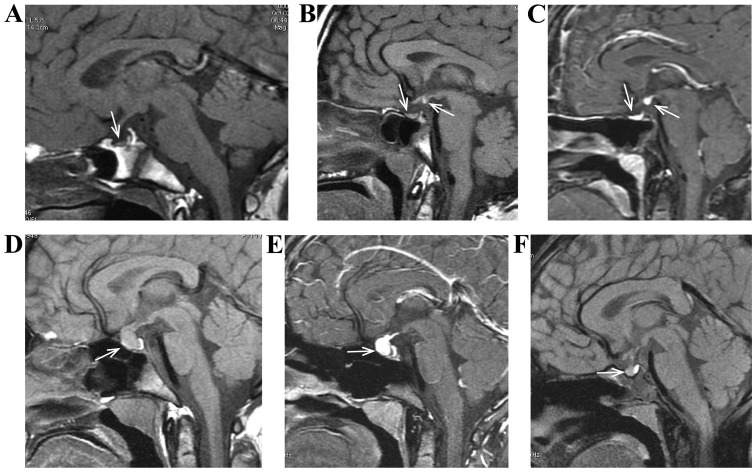
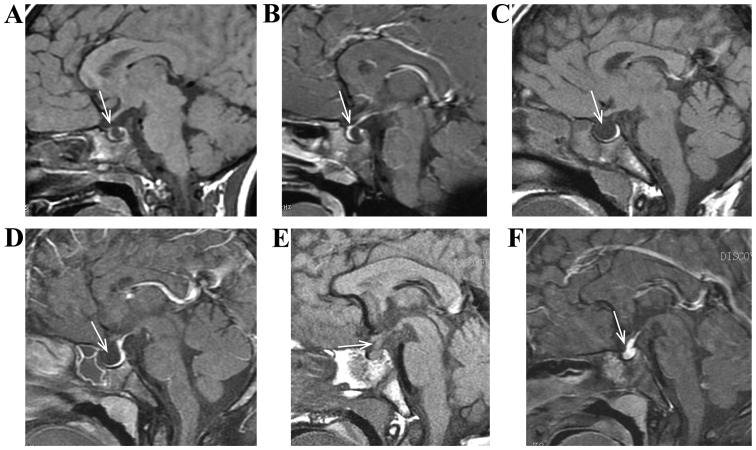
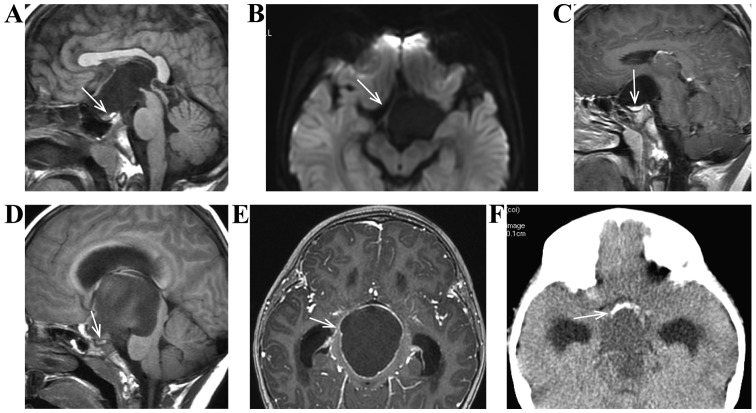
We verified the advantages of using magnetic resonance imaging (MRI) for improving the diagnostic quality of growth hormone deficiency (GHD) in children with short stature caused by pituitary lesions. Clinical data obtained from 577 GHD patients with short stature caused by pituitary lesions were retrospectively analyzed. There were 354 cases (61.3%) with anterior pituitary dysplasia; 45 cases (7.8%) of pituitary stalk interruption syndrome (PSIS); 15 cases (2.6%) of pituitary hyperplasia due to primary hypothyroidism; 38 cases (6.6%) of Rathke cleft cyst; 68 cases (11.8%) of empty sella syndrome; 16 cases (2.8%) of pituitary invasion from Langerhans cell histiocytosis; 2 cases (0.3%) of sellar regional arachnoid cyst and 39 cases (6.8%) of craniopharyngioma. MRI results showed that the height of anterior pituitary in patients was less than normal. Location, size and signals of posterior pituitary and pituitary stalk were normal in anterior pituitary dysplasia. In all cases pituitary hyperplasia was caused by hypothyroidism. MRI results showed that anterior pituitary was enlarged, and we detected upward apophysis and obvious homogeneous enhancement. There were no pituitary stalk interruption and abnormal signal. We also observed that after hormone replacement therapy the size of pituitary gland was reduced. Anterior pituitary atrophy was observed in Rathke cleft cyst, empty sella syndrome, sellar regional arachnoid cyst and craniopharyngioma. The microstructure of hypophysis and sellar region was studied with MRI. We detected pituitary lesions, and the characteristics of various pituitary diseases of GHD in children with short stature. It was concluded that in children with GHD caused by pituitary lesions, MRI was an excellent method for early diagnosis. This method offers clinical practicability and we believe it can be used for differential diagnosis and to monitor the therapeutic effects.
Keywords: growth hormone deficiency; magnetic resonance imaging; pituitary.
Figures
Similar articles
-
Is Gadolinium Contrast Necessary for Pituitary MRI in the Evaluation of Pediatric Short Stature and Growth Hormone Deficiency?Horm Res Paediatr. 2021;94(5-6):201-210. doi: 10.1159/000519031. Epub 2021 Aug 23. Horm Res Paediatr. 2021. PMID: 34425574
-
Pituitary stalk interruption syndrome: the role of MRI and review of the literature.Neuroradiol J. 2010 Oct;23(5):607-12. doi: 10.1177/197140091002300510. Epub 2010 Oct 31. Neuroradiol J. 2010. PMID: 24148682
-
[Magnetic resonance imaging characteristics and differential diagnosis of common sellar cystic lesions].Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2019 Nov 7;54(11):819-825. doi: 10.3760/cma.j.issn.1673-0860.2019.11.004. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2019. PMID: 31795542 Chinese.
-
Pituitary stalk interruption syndrome and liver cirrhosis associated with diabetes and an inactivating KCNJ11 gene mutation: a case report and literature review.Front Endocrinol (Lausanne). 2023 Dec 13;14:1297146. doi: 10.3389/fendo.2023.1297146. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 38152125 Free PMC article. Review.
-
Magnetic resonance images of 91 children with different causes of short stature: pituitary size reflects growth hormone secretion.Eur J Pediatr. 1997 Oct;156(10):758-63. doi: 10.1007/s004310050707. Eur J Pediatr. 1997. PMID: 9365063 Review.
Cited by
-
Endocrine Disorder in Patients With Craniopharyngioma.Front Neurol. 2021 Dec 2;12:737743. doi: 10.3389/fneur.2021.737743. eCollection 2021. Front Neurol. 2021. PMID: 34925209 Free PMC article. Review.
-
Distinct pituitary hormone levels of 184 Chinese children and adolescents with multiple pituitary hormone deficiency: a single-centre study.BMC Pediatr. 2019 Nov 14;19(1):441. doi: 10.1186/s12887-019-1819-6. BMC Pediatr. 2019. PMID: 31722706 Free PMC article.
-
Single center study of 53 consecutive patients with pituitary stalk lesions.Pituitary. 2018 Dec;21(6):605-614. doi: 10.1007/s11102-018-0914-2. Pituitary. 2018. PMID: 30276501
-
Heterozygous variants in SIX3 and POU1F1 cause pituitary hormone deficiency in mouse and man.Hum Mol Genet. 2023 Jan 13;32(3):367-385. doi: 10.1093/hmg/ddac192. Hum Mol Genet. 2023. PMID: 35951005 Free PMC article.
-
Diversity of Pathological Conditions Affecting Pituitary Stalk.J Clin Med. 2021 Apr 14;10(8):1692. doi: 10.3390/jcm10081692. J Clin Med. 2021. PMID: 33920036 Free PMC article.
References
-
- Wolfsdorf J, Farquhar JW, Rigal WM. Screening tests for growth-hormone deficiency in dwarfism. Lancet. 1967;2:1271–1273. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources