

Anti-nuclear autoantibodies in the general German population: prevalence and lack of association with selected cardiovascular and metabolic disorders-findings of a multicenter population-based study
- PMID: 28587625
- PMCID: PMC5461675
- DOI: 10.1186/s13075-017-1338-5
Anti-nuclear autoantibodies in the general German population: prevalence and lack of association with selected cardiovascular and metabolic disorders-findings of a multicenter population-based study
Abstract
Background: We determined the prevalence of anti-nuclear autoantibodies (ANAs) in the German adult population and examined the association between ANAs and cardiovascular and metabolic disorders.
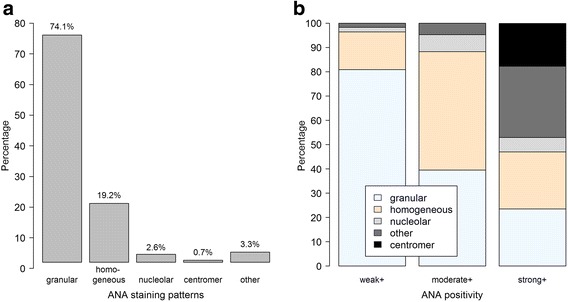
Methods: We used data and blood samples from the pretest phases of the German National Cohort, obtained from six of the 18 study centers (n = 1199). All centers applied standardized instruments including face-to-face interviews, anthropometric measurements and collection of blood samples. Self-reported histories of diabetes mellitus, heart attack and elevated blood cholesterol and/or lipids were recorded. Height, weight and blood pressure were measured. ANAs were detected using a semi-automated system (AKLIDES®; Medipan GmbH, Dahlewitz, Germany). A positive ANA was defined as a titer ≥ 1:80. ANA were classified as weakly (1:80 or 1:160), moderately (1:320 or 1:640) or strongly (≥1:1280) positive. Specific autoantibodies against nuclear antigens were detected with second-step assays according to the ANA staining pattern. Associations between the assessed disorders and ANA positivity and pattern were examined using sex and age-adjusted mixed-effects logistic regression models.
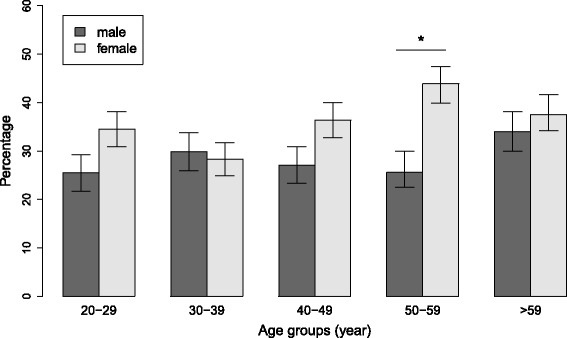
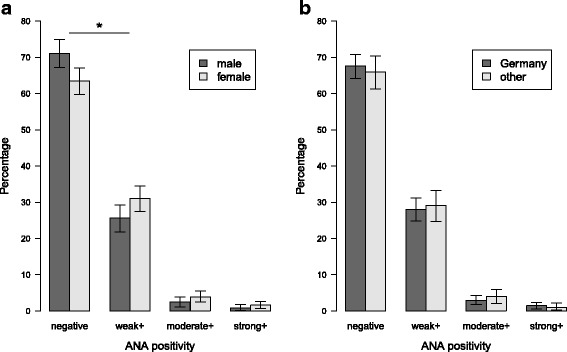
Results: Thirty-three percent (95% confidence interval; 31-36%) of the 1196 participants (measurements could not be obtained from three samples) were ANA positive (titer ≥ 1:80). The proportions of weakly, moderately and strongly positive ANA were 29%, 3.3% and 1.3%, respectively. ANA positivity was more common among women than men across all titers (χ2, p = 0.03). ANA positivity, even when stratified according to height of titer or immunofluorescent pattern, was not associated with diabetes, elevated blood cholesterol and/or lipids, obesity or hypertension. Second-step autoantibody assays were positive in 41 of the 83 samples (49%) tested, with anti-DFS70 (n = 13) and anti-dsDNA (n = 7) being most frequent. These subgroups were too small to test for associations with the disorders assessed.
Conclusions: The prevalence of ANA positivity in the German general population was similar to values reported from other countries. Contrary to other studies, there was no association with selected self-reported and objectively measured cardiovascular and metabolic variables.
Keywords: Anti-nuclear autoantibodies; Diabetes; German National Cohort; Hypertension; Metabolism; Obesity; Population-based study.
Figures
References
-
- O’Sullivan M, McLean-Tooke A, Loh RK. Antinuclear antibody test. Aust Fam Physician. 2013;42:718–21. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
