

Successful Growth Hormone Therapy in Cornelia de Lange Syndrome
- PMID: 28588001
- PMCID: PMC5785645
- DOI: 10.4274/jcrpe.4349
Successful Growth Hormone Therapy in Cornelia de Lange Syndrome
Abstract
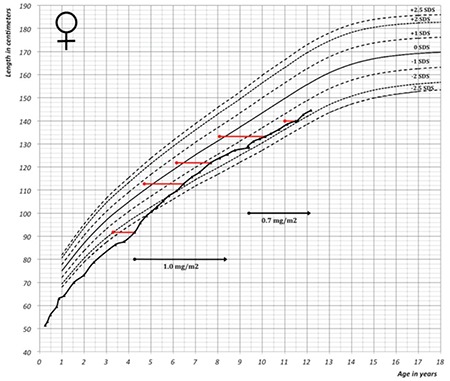
Cornelia de Lange syndrome (CdLS) is a both clinically and genetically heterogeneous syndrome. In its classical form, it is characterised by distinctive facial features, intra-uterine growth retardation, short stature, developmental delay, and anomalies in multiple organ systems. NIPBL, SMC1A, SMC3, RAD21 and HDAC8, all involved in the cohesin pathway, have been identified to cause CdLS. Growth hormone (GH) secretion has been reported as normal, and to our knowledge, there are no reports on the effect of recombinant human GH treatment in CdLS patients. We present a patient born small for gestational age with persistent severe growth retardation [height -3.4 standard deviation score (SDS)] and mild dysmorphic features, who was treated with GH from 4.3 years of age onward and was diagnosed 6 years later with CdLS using whole-exome sequencing. Treatment led to a height gain of 1.6 SDS over 8 years. Treatment was interrupted shortly due to high serum insulin-like growth factor-1 serum values. In conclusion, GH therapy may be effective and safe for short children with CdLS.
Keywords: Cornelia de Lange syndrome; NIPBL whole-exome sequencing.; growth hormone; small for gestational age.
Figures



Similar articles
-
Exome sequencing identifies a novel EP300 frame shift mutation in a patient with features that overlap Cornelia de Lange syndrome.Am J Med Genet A. 2014 Jan;164A(1):251-8. doi: 10.1002/ajmg.a.36237. Epub 2013 Oct 29. Am J Med Genet A. 2014. PMID: 24352918 Review.
-
Severe ipsilateral musculoskeletal involvement in a Cornelia de Lange patient with a novel NIPBL mutation.Eur J Med Genet. 2014 Sep;57(9):503-9. doi: 10.1016/j.ejmg.2014.05.006. Epub 2014 May 27. Eur J Med Genet. 2014. PMID: 24874887
-
A novel mosaic variant on SMC1A reported in buccal mucosa cells, albeit not in blood, of a patient with Cornelia de Lange-like presentation.Cold Spring Harb Mol Case Stud. 2020 Jun 12;6(3):a005322. doi: 10.1101/mcs.a005322. Print 2020 Jun. Cold Spring Harb Mol Case Stud. 2020. PMID: 32532882 Free PMC article.
-
Two novel RAD21 mutations in patients with mild Cornelia de Lange syndrome-like presentation and report of the first familial case.Gene. 2014 Mar 10;537(2):279-84. doi: 10.1016/j.gene.2013.12.045. Epub 2013 Dec 27. Gene. 2014. PMID: 24378232
-
Special cases in Cornelia de Lange syndrome: The Spanish experience.Am J Med Genet C Semin Med Genet. 2016 Jun;172(2):198-205. doi: 10.1002/ajmg.c.31501. Epub 2016 May 10. Am J Med Genet C Semin Med Genet. 2016. PMID: 27164022 Review.
Cited by
-
Disease-associated c-MYC downregulation in human disorders of transcriptional regulation.Hum Mol Genet. 2022 May 19;31(10):1599-1609. doi: 10.1093/hmg/ddab348. Hum Mol Genet. 2022. PMID: 34849865 Free PMC article.
-
Analysis of clinical and genetic characteristics in 10 Chinese individuals with Cornelia de Lange syndrome and literature review.Mol Genet Genomic Med. 2020 Oct;8(10):e1471. doi: 10.1002/mgg3.1471. Epub 2020 Aug 27. Mol Genet Genomic Med. 2020. PMID: 32856424 Free PMC article. Review.
-
Advancing the Clinical and Molecular Understanding of Cornelia de Lange Syndrome: A Multidisciplinary Pediatric Case Series and Review of the Literature.J Clin Med. 2024 Apr 21;13(8):2423. doi: 10.3390/jcm13082423. J Clin Med. 2024. PMID: 38673696 Free PMC article. Review.
-
Two Years of Growth Hormone Therapy in a Child with Severe Short Stature Due to Overlap Syndrome with a Novel SETD5 Gene Mutation: Case Report and Review of the Literature.Genes (Basel). 2025 Jul 23;16(8):859. doi: 10.3390/genes16080859. Genes (Basel). 2025. PMID: 40869907 Free PMC article. Review.
-
A Chinese Case of Cornelia de Lange Syndrome Caused by a Pathogenic Variant in SMC3 and a Literature Review.Front Endocrinol (Lausanne). 2021 Sep 30;12:604500. doi: 10.3389/fendo.2021.604500. eCollection 2021. Front Endocrinol (Lausanne). 2021. PMID: 34659104 Free PMC article. Review.
References
-
- de Lange C. Sur un type nouveau de degenerescence (typus Amstelodamensis) Arch Med Enfants. 1933;36:713–719.
-
- Brachmann W. Ein fall von symmetrischer monodaktylie durch Ulnadefekt, mit symmetrischer flughautbildung, in den ellebeugen, sowie anderen abnormitaten (zwerghaftogkeit, halsrippen, behaarung) Jarb Kinder Phys Erzie. 1916;84:225–235.
-
- Van Allen MI, Filippi G, Siegel-Bartelt J, Yong SL, McGillivray B, Zuker RM, Smith CR, Magee JF, Ritchie S, Toi A, et al. Clinical variability within Brachmann-de Lange syndrome: a proposed classification system. Am J Med Genet. 1993;47:947–958. - PubMed
-
- Boyle MI, Jespersgaard C, Brondum-Nielsen K, Bisgaard AM, Tümer Z. Cornelia de Lange syndrome. Clin Genet. 2015;88:1–12. - PubMed
-
- Kline AD, Barr M, Jackson LG. Growth Manifestations in the Brachmann-Delange Syndrome. Am J Med Genet. 1993;47:1042–1049. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous