

Pituitary Adenoma Apoplexy in an Adolescent: A Case Report and Review of the Literature
- PMID: 28588003
- PMCID: PMC5596809
- DOI: 10.4274/jcrpe.4420
Pituitary Adenoma Apoplexy in an Adolescent: A Case Report and Review of the Literature
Abstract
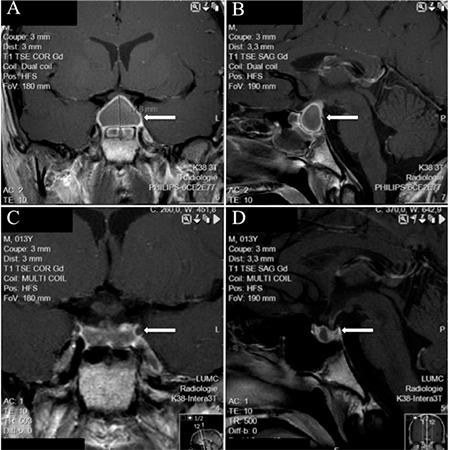
We present a 13-year-old boy who was admitted with complaints of a state of progressive sleepiness and a sudden headache with vomiting and fever. Laboratory testing showed hypoglycemia, multiple pituitary hormonal deficiencies, and an elevated C-reactive protein level. A cranial magnetic resonance imaging (MRI) showed an opaque sphenoid sinus and an intrasellar mass suggesting hemorrhage, so that we suspected pituitary apoplexy (PA) originating from a non-functioning adenoma, although a pituitary abscess could not completely be excluded. The boy was treated with antibiotics, hydrocortisone, and levothyroxine. Due to his rapid clinical improvement, no surgery was performed and we considered the diagnosis of PA as confirmed. At follow-up, the MRI scan showed a small residual lesion. Pituitary deficiencies of growth hormone, adrenocorticotropic hormone (ACTH), thyroid-stimulating hormone, and vasopressin persisted. A literature search of all well-documented cases of PA in children or adolescents (n=30, 13 boys and 17 girls) indicated that this condition is rare below 20 years of age but must be considered when a patient experiences headache with or without visual disturbances, even in the presence of clinical and laboratory signals suggestive of pituitary abscess. MRI neuroimaging is helpful in the differential diagnosis. In both conditions, the possibility of ACTH deficiency should always be considered, investigated, and treated. In cases without severe neuro-ophthalmological deficits and/or with a rapid and positive response to acute medical management, one can abstain from surgical treatment.
Keywords: Pituitary adenoma; adolescents; apoplexy; headache magnetic resonance imaging.; panhypopituitarism; pituitary abscess.
Figures
References
-
- Mindermann T, Wilson CB. Pediatric pituitary adenomas. Neurosurgery. 1995;36:259–269. - PubMed
-
- Oldfield EH, Merrill MJ. Apoplexy of pituitary adenomas: the perfect storm. J Neurosurg. 2015;122:1444–1449. - PubMed
-
- Briet C, Salenave S, Bonneville JF, Laws ER, Chanson P. Pituitary Apoplexy. Endocr Rev. 2015;36:622–645. - PubMed
-
- Dawson BH, Kothandaram P. Acute massive infarction of pituitary adenomas. A study of five patients. J Neurosurg. 1972;37:275–279. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials