

Implantable Cardioverter-Defibrillator Therapy in Arrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy: Predictors of Appropriate Therapy, Outcomes, and Complications
- PMID: 28588093
- PMCID: PMC5669204
- DOI: 10.1161/JAHA.117.006242
Implantable Cardioverter-Defibrillator Therapy in Arrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy: Predictors of Appropriate Therapy, Outcomes, and Complications
Abstract
Background: Arrhythmogenic right ventricular dysplasia/cardiomyopathy is characterized by ventricular arrhythmias and sudden cardiac death. Once the diagnosis is established, risk stratification to determine whether implantable cardioverter-defibrillator (ICD) placement is warranted is critical.
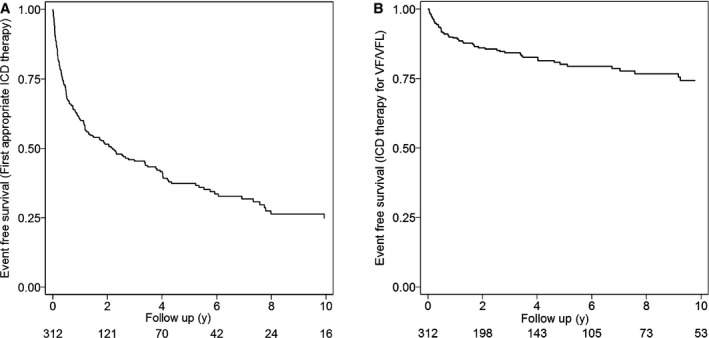
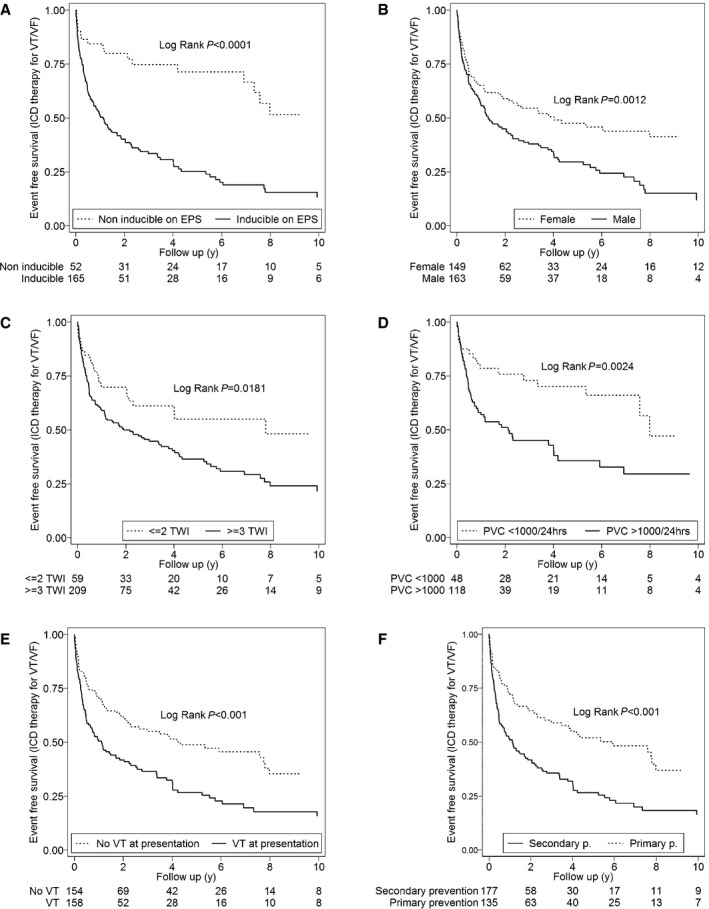
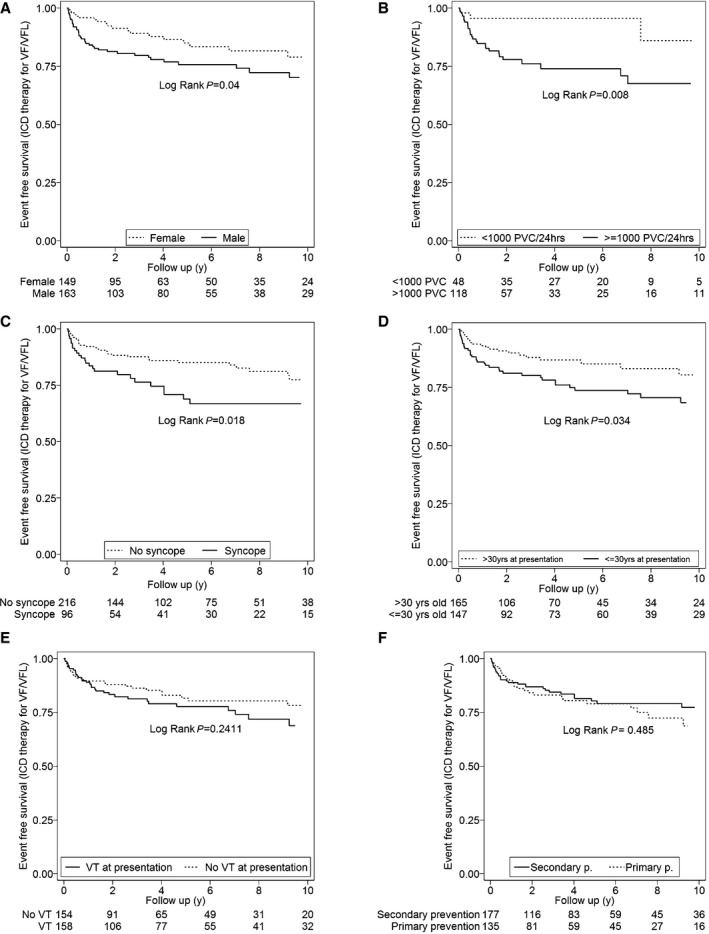
Methods and results: The cohort included 312 patients (163 men, age at presentation 33.6±13.9 years) with definite arrhythmogenic right ventricular dysplasia/cardiomyopathy who received an ICD. Over 8.8±7.33 years, 186 participants (60%) had appropriate ICD therapy and 58 (19%) had an intervention for ventricular fibrillation/flutter. Ventricular tachycardia at presentation (hazard ratio [HR]: 1.86; 95% confidence interval [CI], 1.38-2.49; P<0.001), inducibility on electrophysiology study (HR: 3.14; 95% CI, 1.95-5.05; P<0.001), male sex (HR: 1.62; 95% CI, 1.20-2.19; P=0.001), inverted T waves in ≥3 precordial leads (HR: 1.66; 95% CI, 1.09-2.52; P=0.018), and premature ventricular contraction count ≥1000/24 hours (HR: 2.30; 95% CI, 1.32-4.00; P=0.003) were predictors of any appropriate ICD therapy. Inducibility at electrophysiology study (HR: 2.28; 95% CI, 1.10-4.70; P=0.025) remained as the only predictor after multivariable analysis. The predictors for ventricular fibrillation/flutter were premature ventricular contraction ≥1000/24 hours (HR: 4.39; 95% CI, 1.32-14.61; P=0.016), syncope (HR: 1.85; 95% CI, 1.10-3.11; P=0.021), aged ≤30 years at presentation (HR: 1.76; 95% CI, 1.04-3.00; P<0.036), and male sex (HR: 1.73; 95% CI, 1.01-2.97; P=0.046). Younger age at presentation (HR: 3.14; 95% CI, 1.32-7.48; P=0.010) and high premature ventricular contraction burden (HR: 4.43; 95% CI, 1.35-14.57; P<0.014) remained as independent predictors of ventricular fibrillation/flutter. Complications occurred in 66 participants (21%), and 64 (21%) had inappropriate ICD interventions. Overall mortality was low at 2%, and 4% underwent heart transplantation.
Conclusion: These findings represent an important step in identifying predictors of ICD therapy for potentially fatal ventricular fibrillation/flutter and should be considered when developing a risk stratification model for arrhythmogenic right ventricular dysplasia/cardiomyopathy.
Keywords: arrhythmogenic right ventricular cardiomyopathy/dysplasia; implantable cardioverter defibrillator; sudden cardiac death; tachyarrhythmias; ventricular fibrillation.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
Similar articles
-
Long-Term Clinical Outcome of Arrhythmogenic Right Ventricular Cardiomyopathy in Individuals With a p.S358L Mutation in TMEM43 Following Implantable Cardioverter Defibrillator Therapy.Circ Arrhythm Electrophysiol. 2016 Mar;9(3):e003589. doi: 10.1161/CIRCEP.115.003589. Circ Arrhythm Electrophysiol. 2016. PMID: 26966288
-
Prophylactic implantable defibrillator in patients with arrhythmogenic right ventricular cardiomyopathy/dysplasia and no prior ventricular fibrillation or sustained ventricular tachycardia.Circulation. 2010 Sep 21;122(12):1144-52. doi: 10.1161/CIRCULATIONAHA.109.913871. Epub 2010 Sep 7. Circulation. 2010. PMID: 20823389
-
Long-term follow-up in patients with arrhythmogenic right ventricular cardiomyopathy.J Cardiovasc Electrophysiol. 2012 Jul;23(7):750-6. doi: 10.1111/j.1540-8167.2011.02288.x. Epub 2012 Feb 21. J Cardiovasc Electrophysiol. 2012. PMID: 22353378
-
Implantable cardioverter defibrillators in arrhythmogenic right ventricular dysplasia/cardiomyopathy: patient outcomes, incidence of appropriate and inappropriate interventions, and complications.Circ Arrhythm Electrophysiol. 2013 Jun;6(3):562-8. doi: 10.1161/CIRCEP.113.000392. Epub 2013 May 14. Circ Arrhythm Electrophysiol. 2013. PMID: 23673907 Review.
-
Risk Stratification in Arrhythmogenic Right Ventricular Cardiomyopathy.Circulation. 2017 Nov 21;136(21):2068-2082. doi: 10.1161/CIRCULATIONAHA.117.030792. Circulation. 2017. PMID: 29158215 Free PMC article. Review.
Cited by
-
Long-Term Outcomes Among a Nationwide Cohort of Patients Using an Implantable Cardioverter-Defibrillator: UMBRELLA Study Final Results.J Am Heart Assoc. 2021 Jan 5;10(1):e018108. doi: 10.1161/JAHA.120.018108. Epub 2020 Dec 25. J Am Heart Assoc. 2021. PMID: 33356406 Free PMC article.
-
The Challenges of Diagnosis and Treatment of Arrhythmogenic Cardiomyopathy: Are We there yet?Rev Cardiovasc Med. 2022 Aug 15;23(8):283. doi: 10.31083/j.rcm2308283. eCollection 2022 Aug. Rev Cardiovasc Med. 2022. PMID: 39076647 Free PMC article.
-
2019 HRS/EHRA/APHRS/LAHRS expert consensus statement on catheter ablation of ventricular arrhythmias.J Interv Card Electrophysiol. 2020 Oct;59(1):145-298. doi: 10.1007/s10840-019-00663-3. J Interv Card Electrophysiol. 2020. PMID: 31984466 Free PMC article.
-
Sex Differences in Right Ventricular Dysfunction: Insights From the Bench to Bedside.Front Physiol. 2021 Jan 18;11:623129. doi: 10.3389/fphys.2020.623129. eCollection 2020. Front Physiol. 2021. PMID: 33536939 Free PMC article. Review.
-
Arrhythmogenic Right Ventricular Cardiomyopathy in a Patient Experiencing Out-of-Hospital Ventricular Fibrillation Arrest Twice: Case Report and Review of the Literature.Cureus. 2022 Jan 20;14(1):e21457. doi: 10.7759/cureus.21457. eCollection 2022 Jan. Cureus. 2022. PMID: 35223241 Free PMC article.
References
-
- Corrado D, Link MS, Calkins H. Arrhythmogenic right ventricular cardiomyopathy. N Engl J Med. 2017;376:61–72. - PubMed
-
- Olde Nordkamp LR, Postema PG, Knops RE, van Dijk N, Limpens J, Wilde AA, de Groot JR. Implantable cardioverter‐defibrillator harm in young patients with inherited arrhythmia syndromes: a systematic review and meta‐analysis of inappropriate shocks and complications. Heart Rhythm. 2016;13:443–454. - PubMed
-
- Marcus FI, McKenna WJ, Sherrill D, Basso C, Bauce B, Bluemke DA, Calkins H, Corrado D, Cox MG, Daubert JP, Fontaine G, Gear K, Hauer R, Nava A, Picard MH, Protonotarios N, Saffitz JE, Sanborn DM, Steinberg JS, Tandri H, Thiene G, Towbin JA, Tsatsopoulou A, Wichter T, Zareba W. Diagnosis of arrhythmogenic right ventricular cardiomyopathy/dysplasia: proposed modification of the Task Force Criteria. Eur Heart J. 2010;31:806–814. - PMC - PubMed
-
- Maron BJ, Shen WK, Link MS, Epstein AE, Almquist AK, Daubert JP, Bardy GH, Favale S, Rea RF, Boriani G, Estes NA III, Spirito P. Efficacy of implantable cardioverter‐defibrillators for the prevention of sudden death in patients with hypertrophic cardiomyopathy. N Engl J Med. 2000;342:365–373. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
