

Specific Antibody Deficiency: Controversies in Diagnosis and Management
- PMID: 28588580
- PMCID: PMC5439175
- DOI: 10.3389/fimmu.2017.00586
Specific Antibody Deficiency: Controversies in Diagnosis and Management
Erratum in
-
Corrigendum: Specific Antibody Deficiency: Controversies in Diagnosis and Management.Front Immunol. 2018 Mar 15;9:450. doi: 10.3389/fimmu.2018.00450. eCollection 2018. Front Immunol. 2018. PMID: 29576764 Free PMC article.
Abstract
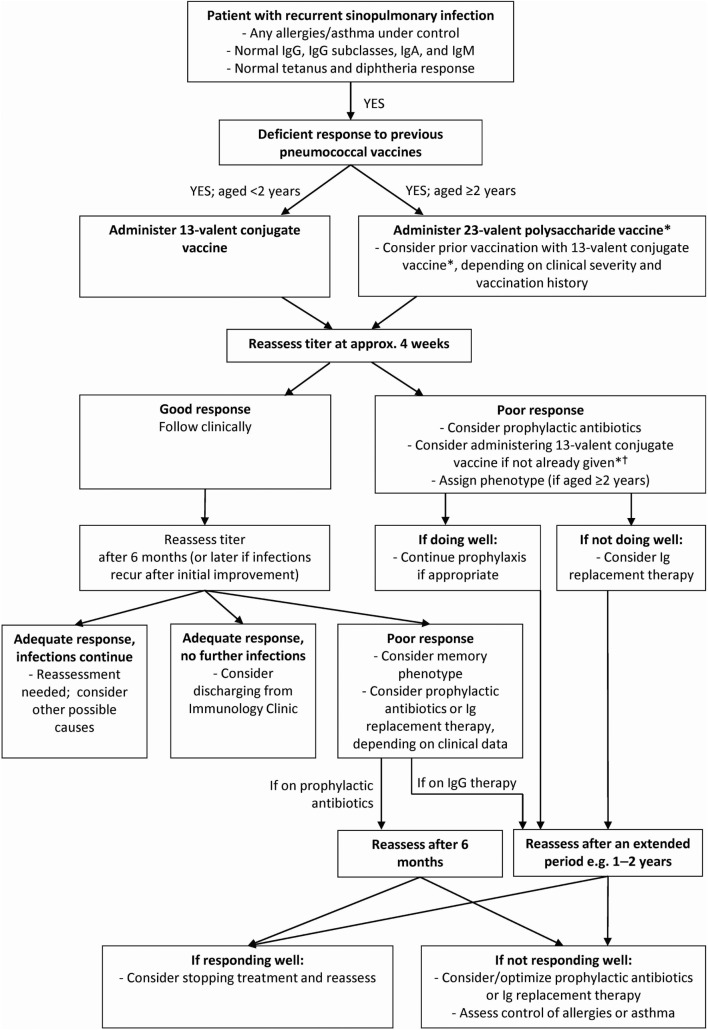
Specific antibody deficiency (SAD) is a primary immunodeficiency disease characterized by normal immunoglobulins (Igs), IgA, IgM, total IgG, and IgG subclass levels, but with recurrent infection and diminished antibody responses to polysaccharide antigens following vaccination. There is a lack of consensus regarding the diagnosis and treatment of SAD, and its clinical significance is not well understood. Here, we discuss current evidence and challenges regarding the diagnosis and treatment of SAD. SAD is normally diagnosed by determining protective titers in response to the 23-valent pneumococcal polysaccharide vaccine. However, the definition of an adequate response to immunization remains controversial, including the magnitude of response and number of pneumococcal serotypes needed to determine a normal response. Confounding these issues, anti-polysaccharide antibody responses are age- and probably serotype dependent. Therapeutic strategies and options for patients with SAD are often based on clinical experience due to the lack of focused studies and absence of a robust case definition. The mainstay of therapy for patients with SAD is antibiotic prophylaxis. However, there is no consensus regarding the frequency and severity of infections warranting antibiotic prophylaxis and no standardized regimens and no studies of efficacy. Published expert guidelines and opinions have recommended IgG therapy, which are supported by observations from retrospective studies, although definitive data are lacking. In summary, there is currently a lack of evidence regarding the efficacy of therapeutic strategies for patients with SAD. We believe that it is best to approach each patient as an individual and progress through diagnostic and therapeutic interventions together with existing practice guidelines.
Keywords: antibody deficiency; diagnosis; immunoglobulin replacement therapy; pneumococcal vaccines; primary immunodeficiency; specific antibody deficiency; treatment.
Figures
References
-
- Soresina A, Mahlaoui N, Wolska B, Edgar D, Ehl S, Thon V, et al. ESID Registry Diagnosis Criteria. (2015). Available from: http://esid.org/Working-Parties/Registry/Diagnosis-criteria
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous