

An update on best practice in the diagnosis and management of post-prostatectomy anastomotic strictures
- PMID: 28588647
- PMCID: PMC5444622
- DOI: 10.1177/1756287217701391
An update on best practice in the diagnosis and management of post-prostatectomy anastomotic strictures
Abstract
Postprostatectomy vesicourethral anastomotic stenosis (VUAS) remains a challenging problem for both patient and urologist. Improved surgical techniques and perioperative identification and treatment of risk factors has led to a decline over the last several decades. High-level evidence to guide management is lacking, primarily relying on small retrospective studies and expert opinion. Endourologic therapies, including dilation and transurethral incision or resection with or without adjunct injection of scar modulators is considered first-line management. Recalcitrant VUAS requires surgical reconstruction of the vesicourethral anastomosis, and in poor surgical candidates, a chronic indwelling catheter or urinary diversion may be the only option. This review provides an update in the diagnosis and management of postprostatectomy VUAS.
Keywords: bladder neck contracture; prostate cancer; radical prostatectomy; urethral stricture; urinary incontinence; vesicourethral anastomotic stenosis.
Conflict of interest statement
Conflict of interest statement: The authors declare that there is no conflict of interest.
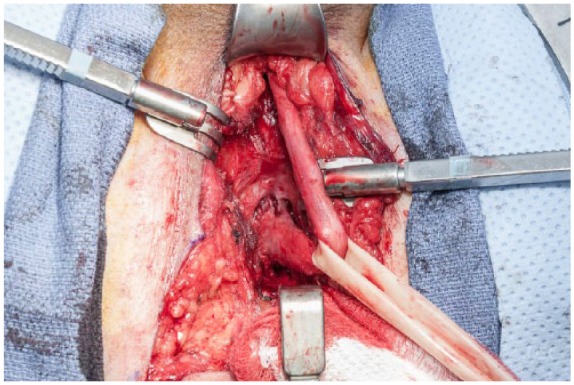
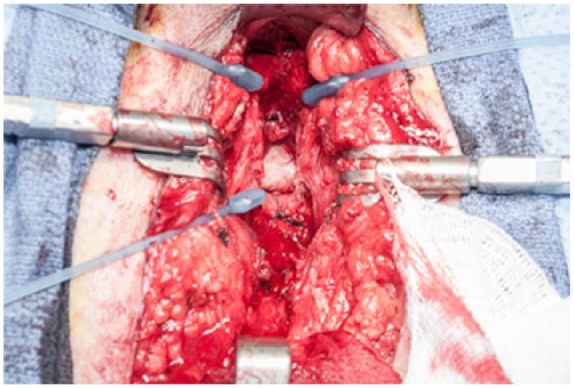
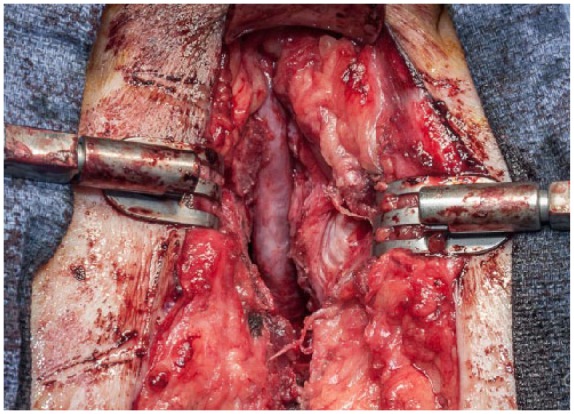
Figures
References
-
- CDC. National Hospital Discharge Survey: 2010 table, Procedures by selected patient characteristics – Number by procedure category and age. 2016.
-
- Halpern JA, Shoag JE, Artis AS, et al. National trends in prostate biopsy and radical prostatectomy volumes following the United States preventative services task force guidelines against prostate-specific antigen screening. JAMA Surg 2016; 152: 192–198. - PubMed
-
- Latini JM, McAninch JW, Brandes SB, et al. SIU/ICUD Consultation on urethral strictures: Epidemiology, etiology, anatomy, and nomenclature of urethral stenoses, strictures, and pelvic fracture urethral disruption injuries. Urology 2014; 83: S1–S7. - PubMed
-
- Elliott SP, Meng MV, Elkin EP, et al. Incidence of urethral stricture after primary treatment for prostate cancer: data From CaPSURE. J Urol 2007; 178: 529–534; discussion 34. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
