

Aetiological pathways to Borderline Personality Disorder symptoms in early adolescence: childhood dysregulated behaviour, maladaptive parenting and bully victimisation
- PMID: 28588894
- PMCID: PMC5457614
- DOI: 10.1186/s40479-017-0060-x
Aetiological pathways to Borderline Personality Disorder symptoms in early adolescence: childhood dysregulated behaviour, maladaptive parenting and bully victimisation
Abstract
Background: Developmental theories for the aetiology of Borderline Personality Disorder (BPD) suggest that both individual features (e.g., childhood dysregulated behaviour) and negative environmental experiences (e.g., maladaptive parenting, peer victimisation) may lead to the development of BPD symptoms during adolescence. Few prospective studies have examined potential aetiological pathways involving these two factors.
Method: We addressed this gap in the literature using data from the Avon Longitudinal Study of Parents and Children (ALSPAC). We assessed mother-reported childhood dysregulated behaviour at 4, 7 and 8 years using the Strengths and Difficulties Questionnaire (SDQ); maladaptive parenting (maternal hitting, punishment, and hostility) at 8 to 9 years; and bully victimisation (child and mother report) at 8, 9 and 10 years. BPD symptoms were assessed at 11 years using the UK Childhood Interview for DSM-IV BPD. Control variables included adolescent depression (assessed with the Short Moods and Feelings Questionnaire-SMFQ) and psychotic symptoms (assessed with the Psychosis-Like Symptoms Interview-PLIKS) at 11 to 14 years, and mother's exposure to family adversity during pregnancy (assessed with the Family Adversity Scale-FAI).
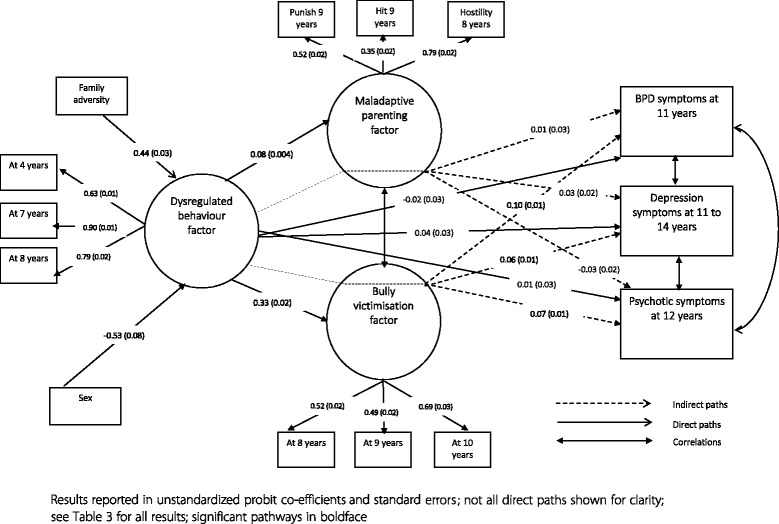
Results: In unadjusted logistic regression analyses, childhood dysregulated behaviour and all environmental risk factors (i.e., family adversity, maladaptive parenting, and bully victimisation) were significantly associated with BPD symptoms at 11 years. Within structural equation modelling controlling for all associations simultaneously, family adversity and male sex significantly predicted dysregulated behaviour across childhood, while bully victimisation significantly predicted BPD, depression, and psychotic symptoms. Children displaying dysregulated behaviour across childhood were significantly more likely to experience maladaptive parenting (β = 0.075, p < 0.001) and bully victimisation (β = 0.327, p < 0.001). Further, there was a significant indirect association between childhood dysregulated behaviour and BPD symptoms via an increased risk of bullying (β = 0.097, p < 0.001). While significant indirect associations between dysregulated behaviour, bully victimisation and depression (β = 0.063, p < 0.001) and psychotic (β = 0.074, p < 0.001) outcomes were also observed, the indirect association was significantly stronger for the BPD outcome (BPD - depression = 0.034, p < 0.01; BPD - psychotic symptoms = 0.023, p < 0.01).
Conclusions: Childhood dysregulated behaviour is associated with BPD in early adolescence via an increased risk of bully victimisation. This suggests that childhood dysregulation may influence the risk of bully victimisation, which in turn influences the development of BPD. Effective interventions should target dysregulated behaviour early on to reduce exposure to environmental risks and the subsequent development of BPD.
Keywords: ALSPAC; BPD; Bullying; Dysregulated behaviour; Harsh parenting; Structural equation modelling.
Figures
Similar articles
-
Sleep Problems in Childhood and Borderline Personality Disorder Symptoms in Early Adolescence.J Abnorm Child Psychol. 2017 Jan;45(1):193-206. doi: 10.1007/s10802-016-0158-4. J Abnorm Child Psychol. 2017. PMID: 27108717 Free PMC article.
-
Prospective study of family adversity and maladaptive parenting in childhood and borderline personality disorder symptoms in a non-clinical population at 11 years.Psychol Med. 2012 Nov;42(11):2405-20. doi: 10.1017/S0033291712000542. Epub 2012 Apr 5. Psychol Med. 2012. PMID: 22475090
-
Bullied by peers in childhood and borderline personality symptoms at 11 years of age: a prospective study.J Child Psychol Psychiatry. 2012 Aug;53(8):846-55. doi: 10.1111/j.1469-7610.2012.02542.x. Epub 2012 Mar 2. J Child Psychol Psychiatry. 2012. PMID: 22380520
-
Parenting behavior and the risk of becoming a victim and a bully/victim: a meta-analysis study.Child Abuse Negl. 2013 Dec;37(12):1091-108. doi: 10.1016/j.chiabu.2013.03.001. Epub 2013 Apr 25. Child Abuse Negl. 2013. PMID: 23623619
-
On the role of oxytocin in borderline personality disorder.Br J Clin Psychol. 2016 Sep;55(3):287-304. doi: 10.1111/bjc.12100. Epub 2015 Nov 30. Br J Clin Psychol. 2016. PMID: 26616386 Review.
Cited by
-
A Measure of Emotional Regulation and Irritability in Children and Adolescents: The Clinical Evaluation of Emotional Regulation-9.J Atten Disord. 2020 Dec;24(14):2002-2011. doi: 10.1177/1087054717737162. Epub 2017 Nov 2. J Atten Disord. 2020. PMID: 29094639 Free PMC article.
-
Early Intervention for Personality Disorder.Focus (Am Psychiatr Publ). 2022 Oct;20(4):402-408. doi: 10.1176/appi.focus.20220062. Epub 2022 Oct 25. Focus (Am Psychiatr Publ). 2022. PMID: 37200874 Free PMC article.
-
Neighbourhood characteristics and the treated incidence rate of borderline personality pathology among young people.Aust N Z J Psychiatry. 2023 Sep;57(9):1263-1270. doi: 10.1177/00048674231157274. Epub 2023 Mar 2. Aust N Z J Psychiatry. 2023. PMID: 36864694 Free PMC article.
-
Prevalence and correlates of emotion dysregulation among children and adolescents in Lebanon: results from a National Survey.BMC Psychiatry. 2024 Oct 17;24(1):698. doi: 10.1186/s12888-024-06169-1. BMC Psychiatry. 2024. PMID: 39420303 Free PMC article.
-
Borderline Personality Disorder: Updates in a Postpandemic World.Focus (Am Psychiatr Publ). 2022 Oct;20(4):337-352. doi: 10.1176/appi.focus.20220057. Epub 2022 Oct 25. Focus (Am Psychiatr Publ). 2022. PMID: 37200886 Free PMC article. Review.
References
-
- Griffiths M. Validity, utility and acceptability of borderline personality disorder diagnosis in childhood and adolescence: survey of psychiatrists. Psychiatrist. 2011;35(1):19–22. doi: 10.1192/pb.bp.109.028779. - DOI
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
