

Mechanistic insights into ADXS11-001 human papillomavirus-associated cancer immunotherapy
- PMID: 28588899
- PMCID: PMC5455112
- DOI: 10.1186/s40661-017-0046-9
Mechanistic insights into ADXS11-001 human papillomavirus-associated cancer immunotherapy
Abstract
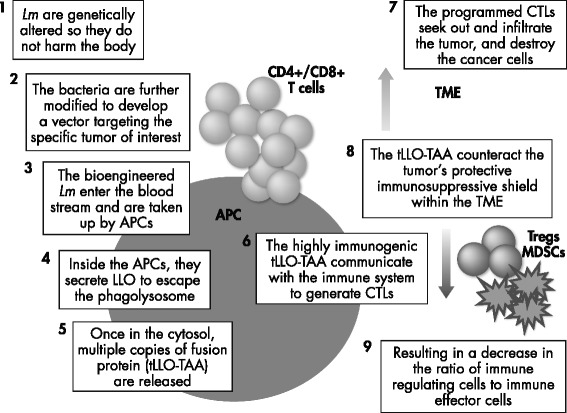
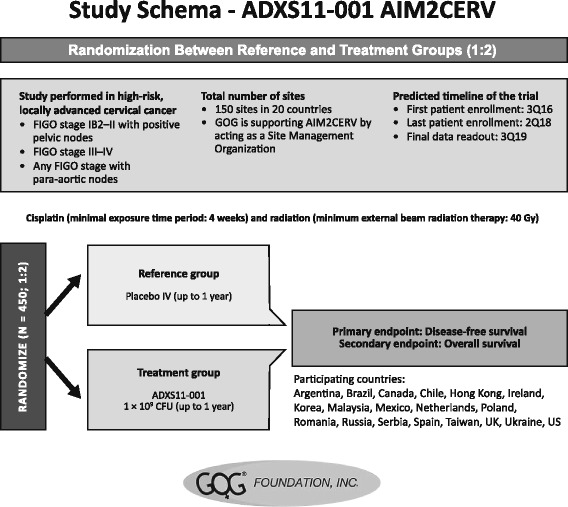
Immune responses to the facultative intracellular bacterium Listeria monocytogenes (Lm) are robust and well characterized. Utilized for decades as a model of host-disease immunology, Lm is well suited for use as an immunotherapeutic bacterial vector for the delivery of foreign antigen. Genetic modification of Lm has been undertaken to create an attenuated organism that is deficient in its master transcriptional regulator, protein-related factor A, and incorporates a truncated, nonhemolytic version of the listeriolysin O (LLO) molecule to ensure its adjuvant properties while also preventing escape of the live organism from the phagolysosome. Delivery of a vaccine construct (Lm-LLO-E7; axalimogene filolisbac [AXAL] or ADXS11-001) in which the modified LLO molecule is fused with the E7 oncoprotein of human papillomavirus type 16 (HPV-16) consistently stimulates strong innate and E7 antigen-specific adaptive immune responses, resulting in reduction of tumor burden in animal cancer models. In the clinical setting, AXAL has shown early promise in phase I/II trials of women with cervical cancer, and several more trials are currently underway to assess the efficacy and safety of this antitumor vaccine in patients with HPV-positive head and neck and anal cancers.
Keywords: ADXS11-001; AXAL; Axalimogene filolisbac; Cancer immunotherapy; Human papillomavirus; Mechanism of action; Vaccine therapy.
Figures


References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
