

Onsite midwife-led birth units (OMBUs) for care around the time of childbirth: a systematic review
- PMID: 28588944
- PMCID: PMC5321346
- DOI: 10.1136/bmjgh-2016-000096
Onsite midwife-led birth units (OMBUs) for care around the time of childbirth: a systematic review
Abstract
Introduction: To ensure timely access to comprehensive emergency obstetric care in low- and middle-income countries, a number of interventions have been employed. This systematic review assesses the effects of onsite midwife-led birth units (OMBUs) embedded within hospitals which provide comprehensive emergency obstetric and newborn care.
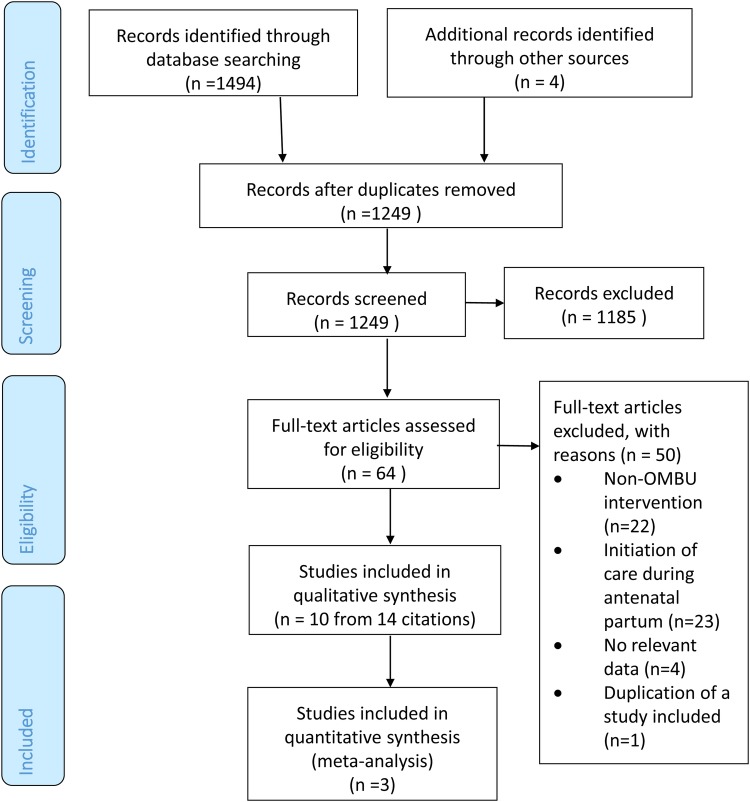
Methods: Both interventional and observational studies that compared OMBUs with standard medical-led obstetric care were eligible for inclusion. Cochrane Central Register of Controlled Trials, PubMed/Medline, EMBASE, CINAHL, Science Citation and Social Sciences Citation Index, Global Health Library and one Chinese database were searched. Meta-analysis was conducted to synthesise data from randomised controlled trials (RCTs). Findings of observational studies were summarised by forest plots with brief narratives.
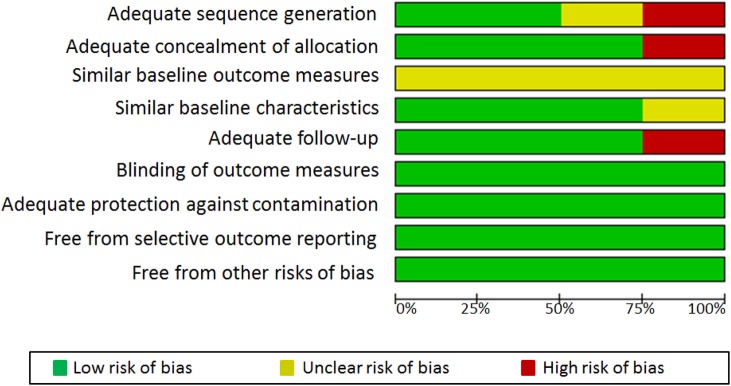
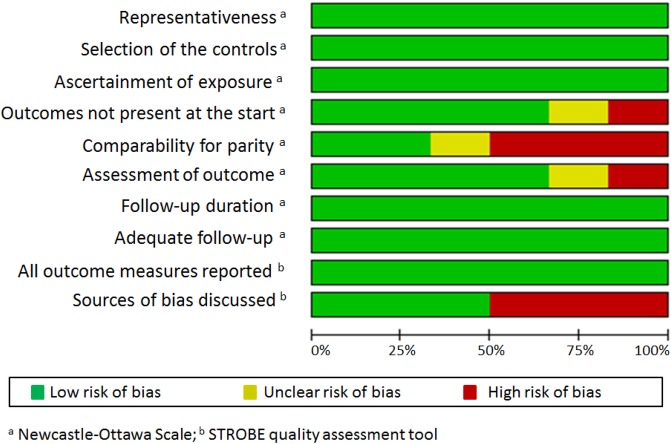
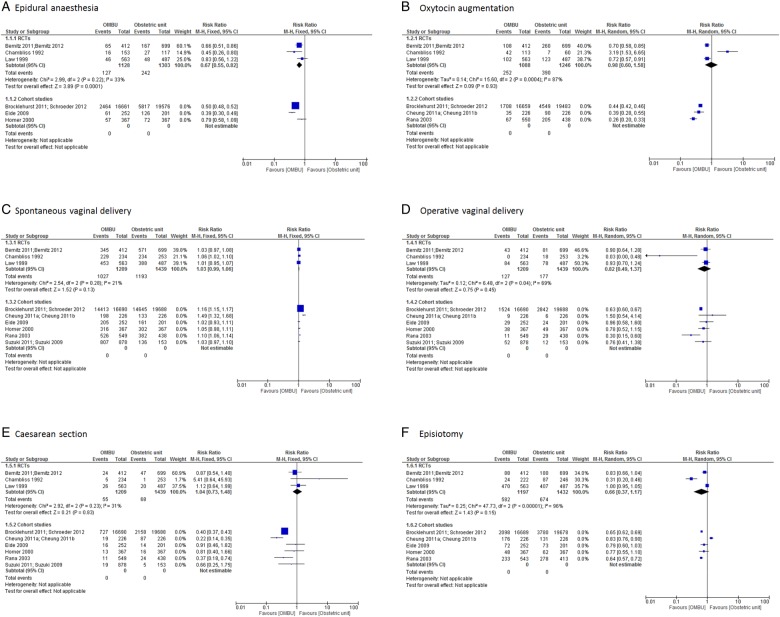
Results: Three RCTs, one controlled before-and-after study and six cohort studies were included. There were no or very few maternal and perinatal deaths in either OMBUs or standard obstetric units, with no significant differences between the two. Women giving birth in OMBUs were less likely to use epidural analgesia (risk ratio (RR) 0.67, 95% CI 0.55 to 0.82; three trials, n=2431). The UK national cohort study and two other cohorts in China and Nepal found less oxytocin augmentation, more spontaneous vaginal deliveries, fewer caesarean sections and fewer episiotomies performed in OMBUs than in standard obstetric units. These differences were not statistically significant in RCTs and the remaining cohorts. One study investigated satisfaction with midwife-led birth care among women and midwives, with positive findings in both groups favouring OMBUs. In addition, two studies found that the total cost of birth was lower in OMBUs than in standard obstetric units.
Conclusions: OMBUs could be an alternative model for providing safe and cost-effective childbirth care, which may be particularly important in low- and middle-income countries to meet the growing demand for facility-based birth for low-risk women and improve efficiency of health systems.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- World Health Organization. The World Health Report 2005: make every mother and child count. Geneva: World Health Organization, 2005.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources