

Determinants of morbidity and mortality following emergency abdominal surgery in children in low-income and middle-income countries
- PMID: 28588977
- PMCID: PMC5321375
- DOI: 10.1136/bmjgh-2016-000091
Determinants of morbidity and mortality following emergency abdominal surgery in children in low-income and middle-income countries
Erratum in
-
Correction: Determinants of morbidity and mortality following emergency abdominal surgery in children in low-income and middleincome countries.BMJ Glob Health. 2017 Jan 30;2(1):bmjgh-2016-000091corr1. doi: 10.1136/bmjgh-2016-000091corr1. eCollection 2017. BMJ Glob Health. 2017. PMID: 28608871 Free PMC article.
Abstract
Background: Child health is a key priority on the global health agenda, yet the provision of essential and emergency surgery in children is patchy in resource-poor regions. This study was aimed to determine the mortality risk for emergency abdominal paediatric surgery in low-income countries globally.
Methods: Multicentre, international, prospective, cohort study. Self-selected surgical units performing emergency abdominal surgery submitted prespecified data for consecutive children aged <16 years during a 2-week period between July and December 2014. The United Nation's Human Development Index (HDI) was used to stratify countries. The main outcome measure was 30-day postoperative mortality, analysed by multilevel logistic regression.
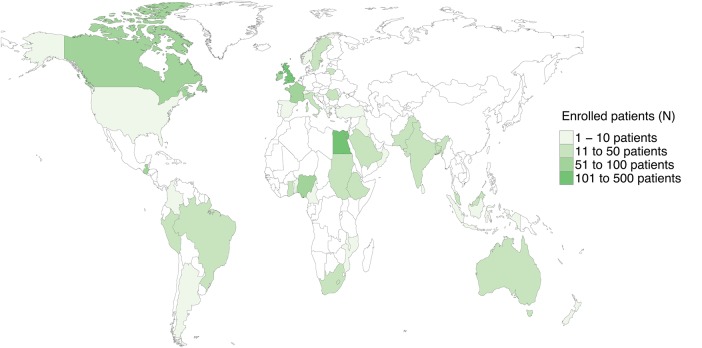
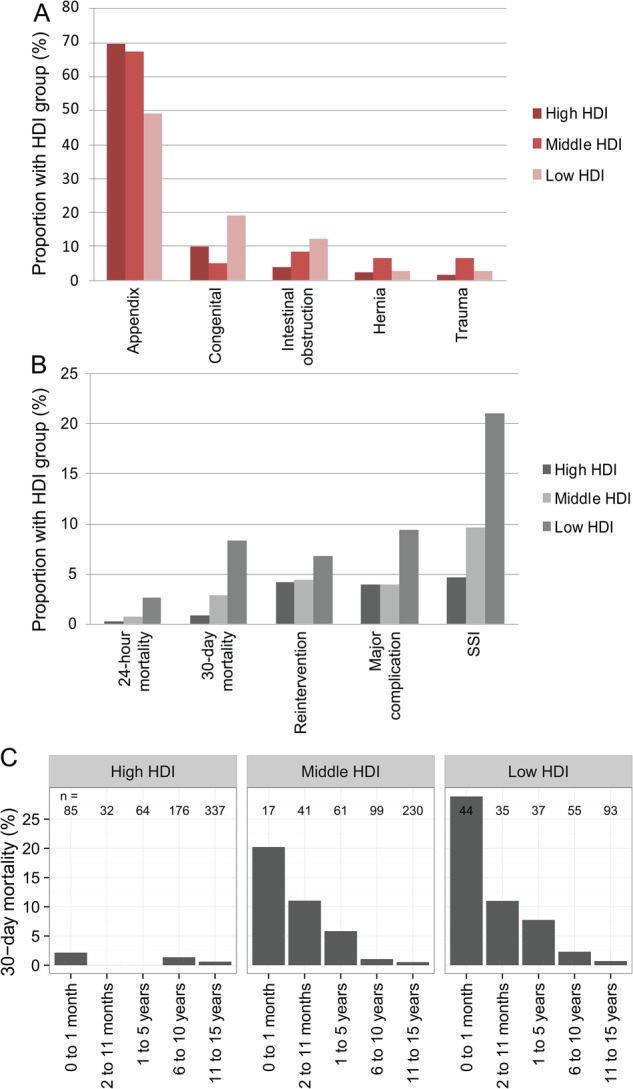
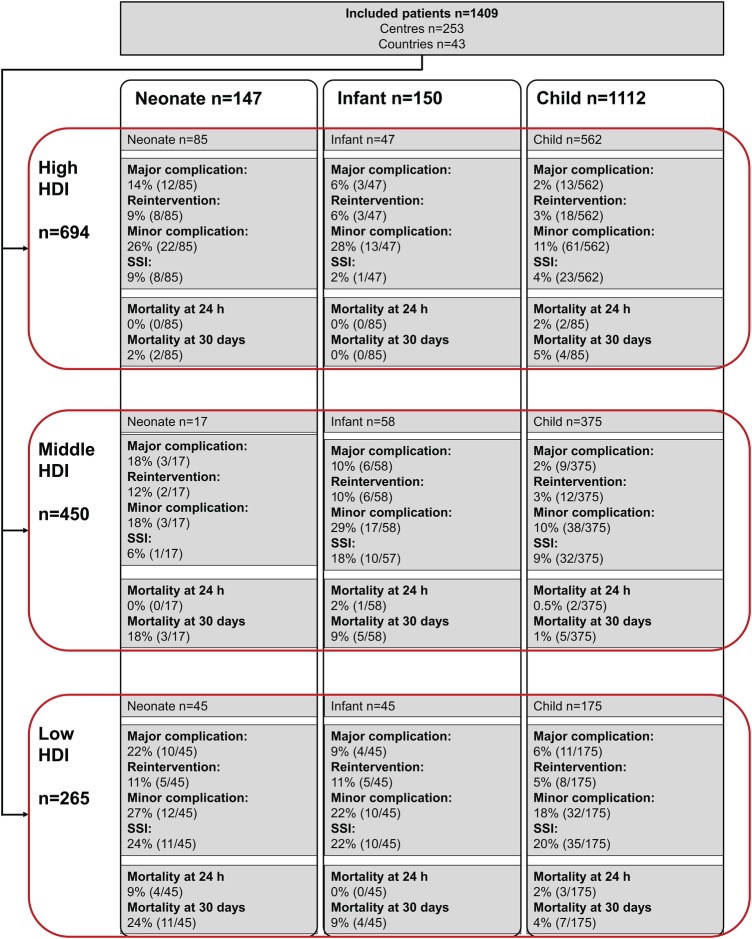
Results: This study included 1409 patients from 253 centres in 43 countries; 282 children were under 2 years of age. Among them, 265 (18.8%) were from low-HDI, 450 (31.9%) from middle-HDI and 694 (49.3%) from high-HDI countries. The most common operations performed were appendectomy, small bowel resection, pyloromyotomy and correction of intussusception. After adjustment for patient and hospital risk factors, child mortality at 30 days was significantly higher in low-HDI (adjusted OR 7.14 (95% CI 2.52 to 20.23), p<0.001) and middle-HDI (4.42 (1.44 to 13.56), p=0.009) countries compared with high-HDI countries, translating to 40 excess deaths per 1000 procedures performed.
Conclusions: Adjusted mortality in children following emergency abdominal surgery may be as high as 7 times greater in low-HDI and middle-HDI countries compared with high-HDI countries. Effective provision of emergency essential surgery should be a key priority for global child health agendas.
Trial registration number: NCT02179112; Pre-results.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical