

Efficacy of three feeding regimens for home-based management of children with uncomplicated severe acute malnutrition: a randomised trial in India
- PMID: 28588982
- PMCID: PMC5321385
- DOI: 10.1136/bmjgh-2016-000144
Efficacy of three feeding regimens for home-based management of children with uncomplicated severe acute malnutrition: a randomised trial in India
Abstract
Objective: To assess the efficacy of ready-to-use therapeutic food (RUTF), centrally produced RUTF (RUTF-C) or locally prepared RUTF (RUTF-L) for home-based management of uncomplicated severe acute malnutrition (SAM) compared with micronutrient-enriched (augmented) energy-dense home-prepared foods (A-HPF, the comparison group).
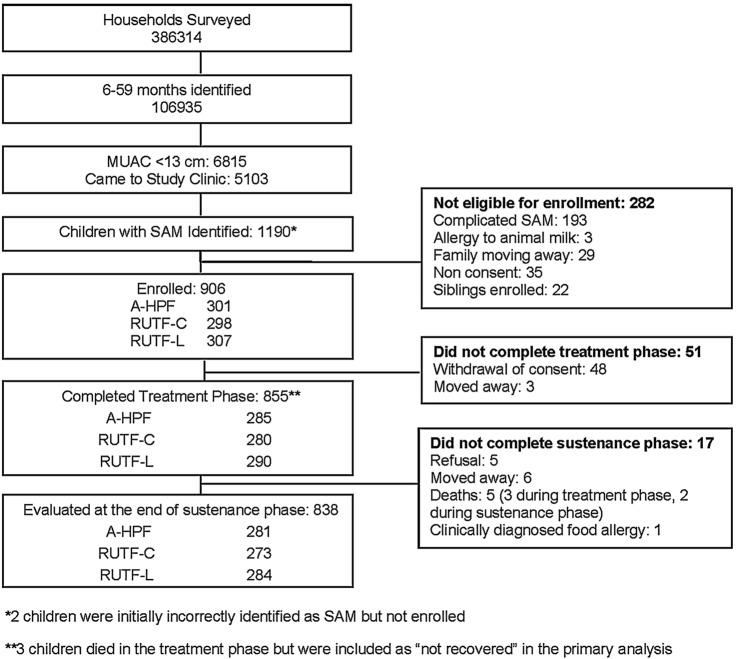
Methods: In an individually randomised multicentre trial, we enrolled 906 children aged 6-59 months with uncomplicated SAM. The children enrolled were randomised to receive RUTF-C, RUTF-L or A-HPF. We provided foods, counselling and feeding support until recovery or 16 weeks, whichever was earlier and measured outcomes weekly (treatment phase). We subsequently facilitated access to government nutrition services and measured outcomes once 16 weeks later (sustenance phase). The primary outcome was recovery during treatment phase (weight-for-height ≥-2 SD and absence of oedema of feet).
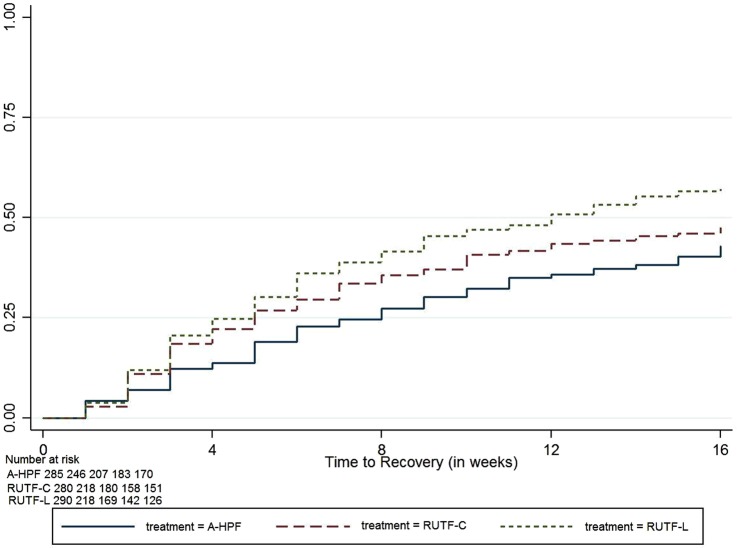
Results: Recovery rates with RUTF-L, RUTF-C and A-HPF were 56.9%, 47.5% and 42.8%, respectively. The adjusted OR was 1.71 (95% CI 1.20 to 2.43; p=0.003) for RUTF-L and 1.28 (95% CI 0.90 to 1.82; p=0.164) for RUTF-C compared with A-HPF. Weight gain in the RUTF-L group was higher than in the A-HPF group (adjusted difference 0.90 g/kg/day, 95% CI 0.30 to 1.50; p=0.003). Time to recovery was shorter in both RUTF groups. Morbidity was high and similar across groups. At the end of the study, the proportion of children with weight-for-height Z-score (WHZ) >-2 was similar (adjusted OR 1.12, 95% CI 0.74 to 1.95; p=0.464), higher for moderate malnutrition (WHZ<-2 and ≥-3; adjusted OR 1.46, 95% CI 1.02 to 2.08; p=0.039), and lower for those with SAM (adjusted OR 0.58, 95% CI 0.40 to 0.85; p=0.005) in the RUTF-L when compared with the A-HPF group.
Conclusions: This first randomised trial comparing options for home management of uncomplicated SAM confirms that RUTF-L is more efficacious than A-HPF at home. Recovery rates were lower than in African studies, despite longer treatment and greater support for feeding.
Trial registration number: NCT01705769; Pre-results.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest Form at http://www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare that RB and SY are staff members of the WHO.
Figures
References
-
- Ministry of Women and Child Development, Government of India. Rapid Survey on Children, 2013–2014: India Fact Sheet. http://wcd.nic.in/issnip/National_Fact%20sheet_RSOC%20_02-07-2015.pdf.
-
- World Health Organization. Joint Child Malnutrition Estimates (UNICEF-WHO-WB): Regional estimates for prevalence and number affected for wasting and severe wasting (2014). http://apps.who.int/gho/data/view.wrapper.nutrition-1-5?lang=en&showonly...
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical