Vaginal Ewing Sarcoma: An Uncommon Clinical Entity in Pediatric Patients
- PMID: 28589056
- PMCID: PMC5433652
- DOI: 10.4103/jcis.JCIS_96_16
Vaginal Ewing Sarcoma: An Uncommon Clinical Entity in Pediatric Patients
Abstract
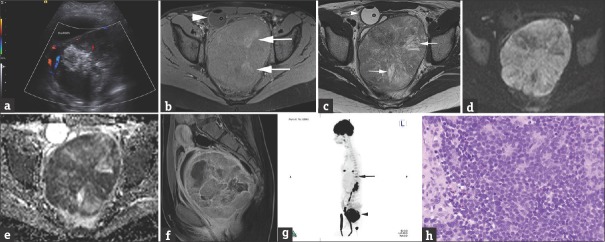
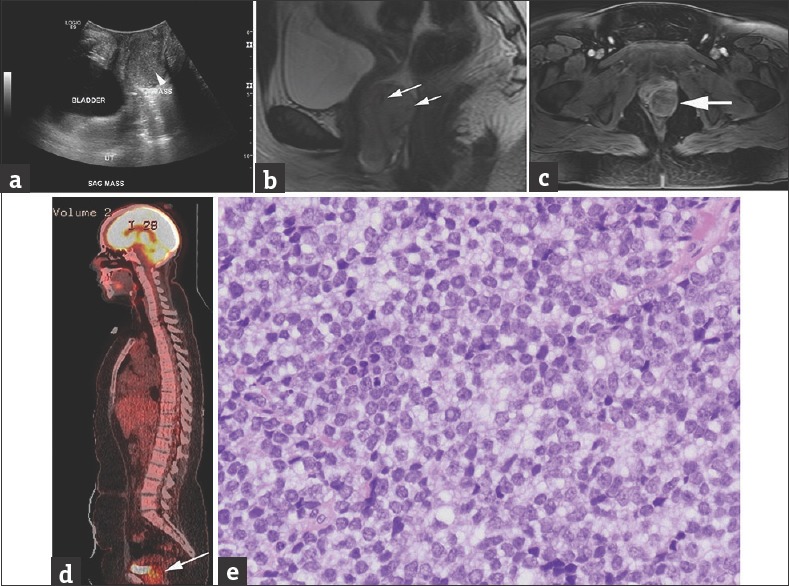
Ewing sarcoma, including classical Ewing sarcoma of the bone and primitive neuroectodermal tumors arising in bone or extraosseous primary sites, is a highly aggressive childhood neoplasm. We present two cases of Ewing sarcoma arising from the vagina in young girls. Previously reported cases in literature focused on their pathologic rather than radiographic features. We describe the spectrum of multimodality imaging appearances of Ewing sarcoma at this unusual primary site. Awareness of vaginal Ewing tumors may facilitate prompt diagnosis and lead to a different surgical approach than the more commonly encountered vaginal rhabdomyosarcoma.
Keywords: Ewing sarcoma; pediatric; vaginal.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- de Alava E, Lessnick SL, Sorensen PH. WHO Classification of Tumours of Soft Tissue and Bone. Lyon: IARC Press; 2013. Ewing sarcoma; pp. 305–9.
-
- Murphey MD, Senchak LT, Mambalam PK, Logie CI, Klassen-Fischer MK, Kransdorf MJ. From the radiologic pathology archives: Ewing sarcoma family of tumors: Radiologic-pathologic correlation. Radiographics. 2013;33:803–31. - PubMed
-
- Bancalari E, de Álava E, Tardío JC. Primary vaginal Ewing sarcoma: Case report and review of the literature. Int J Surg Pathol. 2012;20:305–10. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources