

Discharge or admit? Emergency department management of incidental pulmonary embolism in patients with cancer: a retrospective study
- PMID: 28589462
- PMCID: PMC5461224
- DOI: 10.1186/s12245-017-0144-9
Discharge or admit? Emergency department management of incidental pulmonary embolism in patients with cancer: a retrospective study
Abstract
Background: Hospitalization and early anticoagulation therapy remain standard care for patients who present to the emergency department (ED) with pulmonary embolism (PE). For PEs discovered incidentally, however, optimal therapeutic strategies are less clear-and all the more so when the patient has cancer, which is associated with a hypercoagulable state that exacerbates the threat of PE.
Methods: We conducted a retrospective review of a historical cohort of patients with cancer and incidental PE who were referred for assessment to the ED in an institution whose standard of care is outpatient treatment of selected patients and use of low-molecular-weight heparin for anticoagulation. Eligible patients had received a diagnosis of incidental PE upon routine contrast enhanced chest CT for cancer staging. Survival data was collected at 30 days and 90 days from the date of ED presentation and at the end of the study.
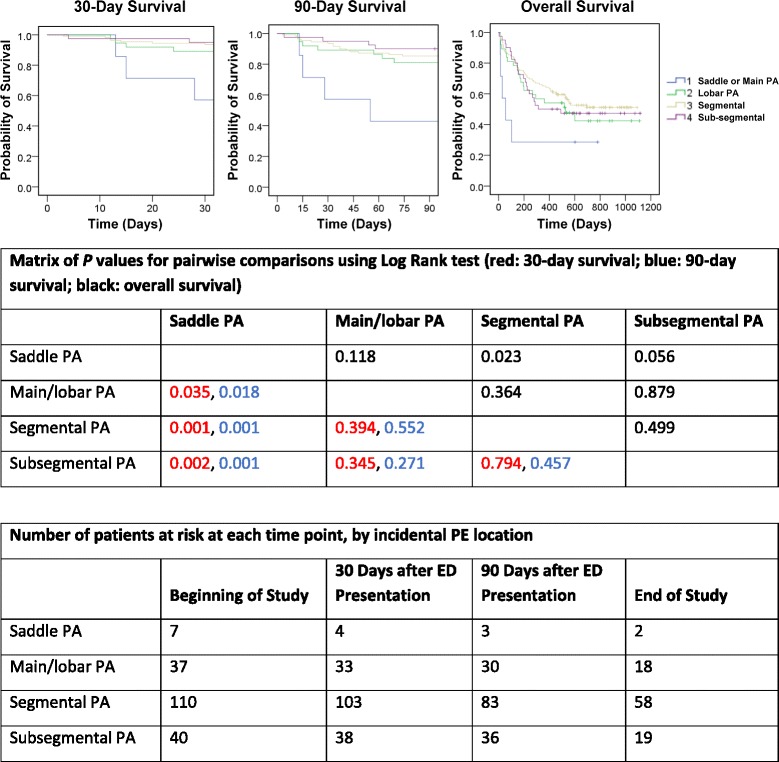
Results: We identified 193 patients, 135 (70%) of whom were discharged and 58 (30%) of whom were admitted to the hospital. The 30-day survival rate was 92% overall, 99% for the discharged patients and 76% for admitted patients. Almost all (189 patients, 98%) commenced anticoagulation therapy in the ED; 170 (90%) of these received low-molecular-weight heparin. Patients with saddle pulmonary artery incidental PEs were more likely to die within 30 days (43%) than were those with main or lobar (11%), segmental (6%), or subsegmental (5%) incidental PEs. In multivariate analysis, Charlson comorbidity index (age unadjusted), hypoxemia, and incidental PE location (P = 0.004, relative risk 33.5 (95% CI 3.1-357.4, comparing saddle versus subsegmental PE) were significantly associated with 30-day survival. Age, comorbidity, race, cancer stage, tachycardia, hypoxemia, and incidental PE location were significantly associated with hospital admission.
Conclusions: Selected cancer patients presenting to the ED with incidental PE can be treated with low-molecular-weight heparin anticoagulation and safely discharged. Avoidance of unnecessary hospitalization may decrease in-hospital infections and death, reduce healthcare costs, and improve patient quality of life. Because the natural history and optimal management of this condition is not well described, information supporting the creation of straightforward evidence-based practice guidelines for ED teams treating this specialized patient population is needed.
Keywords: Cancer; Emergency; Incidental pulmonary embolism; Outpatient.
Figures
Similar articles
-
Discharge from the emergency department and outpatient clinic in cancer patients with acute symptomatic and incidental pulmonary embolism: A multicenter retrospective cohort study.Thromb Res. 2024 Jan;233:181-188. doi: 10.1016/j.thromres.2023.12.003. Epub 2023 Dec 13. Thromb Res. 2024. PMID: 38101191
-
Impact of relative contraindications to home management in emergency department patients with low-risk pulmonary embolism.Ann Am Thorac Soc. 2015 May;12(5):666-73. doi: 10.1513/AnnalsATS.201411-548OC. Ann Am Thorac Soc. 2015. PMID: 25695933 Free PMC article.
-
Frequency and Characteristics of Incidental Pulmonary Embolism in Cancer Patients: A Retrospective Study at a Large Oncology Center in Saudi Arabia.Gulf J Oncolog. 2020 Sep;1(34):26-30. Gulf J Oncolog. 2020. PMID: 33431359
-
Management of incidental pulmonary embolism.Eur Respir J. 2017 Jun 29;49(6):1700275. doi: 10.1183/13993003.00275-2017. Print 2017 Jun. Eur Respir J. 2017. PMID: 28663318 Review.
-
Overdiagnosis of pulmonary embolism: definition, causes and implications.Breathe (Sheff). 2019 Mar;15(1):46-53. doi: 10.1183/20734735.0339-2018. Breathe (Sheff). 2019. PMID: 30838059 Free PMC article. Review.
Cited by
-
Saddle Pulmonary Embolism in Patients with Cancer in the Era of Incidental Events: Clinical Findings and Outcomes in a Single Centre Cohort.TH Open. 2022 Sep 12;6(3):e267-e275. doi: 10.1055/s-0042-1755605. eCollection 2022 Jul. TH Open. 2022. PMID: 36299808 Free PMC article.
-
Incidental pulmonary embolism in oncology patients with current macroscopic malignancy: incidence in different tumour type and impact of delayed treatment on survival outcome.Br J Radiol. 2018 Jul;91(1088):20170806. doi: 10.1259/bjr.20170806. Epub 2018 May 10. Br J Radiol. 2018. PMID: 29688026 Free PMC article.
-
Cutaneous Microembolism of Fingers and Toes.Open Access Maced J Med Sci. 2018 Jan 3;6(1):166-169. doi: 10.3889/oamjms.2018.025. eCollection 2018 Jan 25. Open Access Maced J Med Sci. 2018. PMID: 29484019 Free PMC article. Review.
-
Oncology-related emergencies discharged from the emergency department.Singapore Med J. 2025 Feb 1;66(2):97-101. doi: 10.4103/singaporemedj.SMJ-2021-368. Epub 2023 May 2. Singapore Med J. 2025. PMID: 37171437 Free PMC article.
-
Validation of the EPIPHANY index for predicting risk of serious complications in cancer patients with incidental pulmonary embolism.Support Care Cancer. 2018 Oct;26(10):3601-3607. doi: 10.1007/s00520-018-4235-9. Epub 2018 May 4. Support Care Cancer. 2018. PMID: 29725804
References
-
- Fermann GJ, Erkens PM, Prins MH, Wells PS, Pap AF, Lensing AW. Treatment of pulmonary embolism with rivaroxaban: outcomes by simplified pulmonary embolism severity index score from a post hoc analysis of the EINSTEIN PE study. Acad Emerg Med. 2015;22(3):299–307. doi: 10.1111/acem.12615. - DOI - PMC - PubMed
-
- Torbicki A, Perrier A, Konstantinides S, Agnelli G, Galie N, Pruszczyk P, et al. Guidelines on the diagnosis and management of acute pulmonary embolism: the Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC) Eur Heart J. 2008;29(18):2276–2315. doi: 10.1093/eurheartj/ehn310. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
