

Losartan for the nephropathy of sickle cell anemia: A phase-2, multicenter trial
- PMID: 28589652
- PMCID: PMC5546943
- DOI: 10.1002/ajh.24810
Losartan for the nephropathy of sickle cell anemia: A phase-2, multicenter trial
Abstract
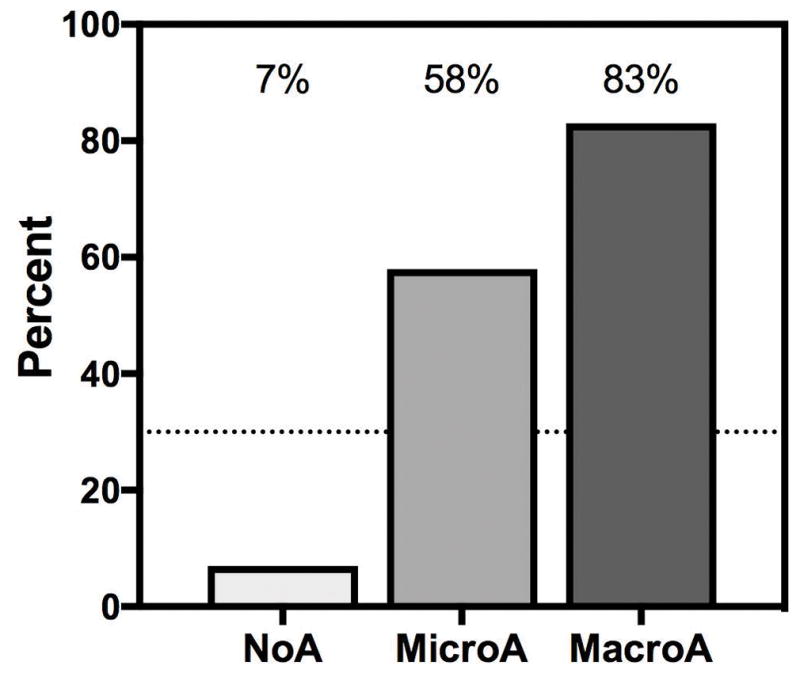
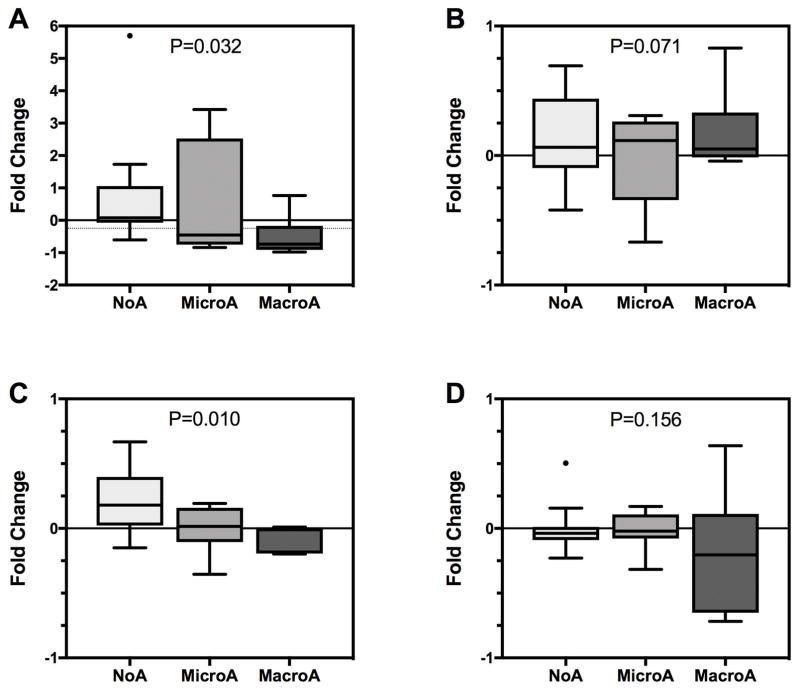
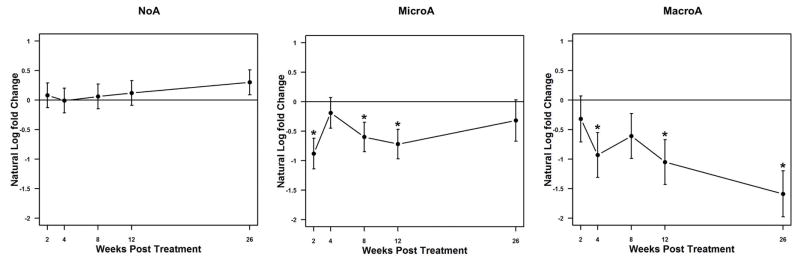
Nephropathy is a common and progressive complication of sickle cell anemia (SCA). In SCA mice, we found that hyperangiotensinemia in the absence of hypertension underlies nephropathy, and its downregulation by losartan, an angiotensin-II-receptor-1 blocker, reduced albuminuria and progression of nephropathy. Therefore, we performed a phase-2 trial of oral losartan, given for 6 months, to explore whether it reduced albuminuria in children and adults with SCA. Participants were allocated to groups defined by class of baseline urinary albumin-to-creatinine ratio (UACR): no albuminuria (NoA), microalbuminuria (MicroA), and macroalbuminuria (MacroA). The primary endpoint was a ≥25% reduction UACR from baseline. There were 32 evaluable participants (mean age 24 years; NoA = 14, MicroA = 12, MacroA = 6). The primary endpoint was met in 83% of the MacroA group (P < 0.0001) and 58% of the MicroA group (P < 0.0001). Median fold-change in UACR was -0.74 for MacroA and -0.46 for MicroA. In MacroA and MicroA, UACR classification improved in 50% but worsened in 11%. Urine osmolality and estimated glomerular filtration rate (eGFR) did not change significantly. Losartan was discontinued in three participants [leg cramps, N = 1; decline in eGFR >25% (142➝104 mL/minute/1.73 m2 ), N = 1; rise in serum creatinine >50% (0.2➝0.3 mg/dL), N = 1]. Albuminuria was associated with diastolic dysfunction and impaired functional capacity, although cardiopulmonary status was unchanged after 6 months of losartan therapy. In summary, losartan decreased urinary albumin excretion in most participants with albuminuria. Those with macroalbuminuria had the greatest benefit. This study forms the basis for a phase-3, randomized, placebo-controlled trial of losartan for the nephropathy of SCA.
© 2017 Wiley Periodicals, Inc.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous