

Ethanol Interactions With Dexmethylphenidate and dl-Methylphenidate Spheroidal Oral Drug Absorption Systems in Healthy Volunteers
- PMID: 28590363
- PMCID: PMC5484776
- DOI: 10.1097/JCP.0000000000000721
Ethanol Interactions With Dexmethylphenidate and dl-Methylphenidate Spheroidal Oral Drug Absorption Systems in Healthy Volunteers
Abstract
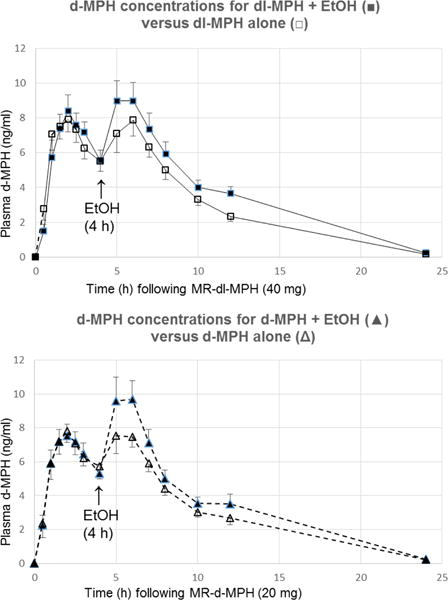
Background/purpose: Ethanol coadministered with immediate-release dl-methylphenidate (dl-MPH) or dexmethylphenidate (d-MPH) significantly increases the geomean maximum plasma concentration (Cmax) of d-MPH 22% and 15%, respectively, and elevates overall drug exposure and psychostimulant effects. We asked the question: Are these ethanol-MPH interactions based more fundamentally on (1) inhibition of postabsorption d-MPH metabolism or (2) acceleration of MPH formulation gastric dissolution by ethanol in the stomach? This was investigated using the pulsatile, distinctly biphasic, spheroidal oral drug absorption systems of dl-MPH and d-MPH.
Methods: In a randomized, 4-way crossover study, 14 healthy subjects received pulsatile dl-MPH (40 mg) or d-MPH (20 mg), with or without ethanol (0.6 g/kg), dosed 4 hours later. These 4 hours allowed the delayed-release second MPH pulse to reach a more distal region of the gut to preclude gastric biopharmaceutical influences. Plasma was analyzed using a highly sensitive chiral method. Subjective/physiological effects were recorded.
Findings/results: Ethanol increased the second pulse of d-MPH Cmax for dl-MPH by 35% (P < 0.01) and the partial area under the plasma concentration curve from 4 to 8 hours by 25% (P < 0.05). The respective values for enantiopure d-MPH were 27% (P = 0.001) and 20% (P < 0.01). The carboxylesterase 1-mediated transesterification metabolite ethylphenidate served as a biomarker for coexposure. Ethanol significantly potentiated stimulant responses to either formulation.
Implications/conclusions: These findings support drug dispositional interactions between ethanol and MPH as dominant over potential biopharmaceutical considerations. Understanding the pharmacology underlying the frequent coabuse of MPH-ethanol provides rational guidance in the selection of first-line pharmacotherapy for comorbid attention-deficit/hyperactivity disorder-alcohol use disorder.
Figures

References
-
- Levin FR, Kleber HD. Attention-deficit hyperactivity disorder and substance abuse: relationships and implications for treatment. Harv Rev Psychiatry. 1995;2:246–58. - PubMed
-
- Barrett SP, Pihl RO. Oral methylphenidate-alcohol co-abuse. J Clin Psychopharmacol. 2002;22:33–34. - PubMed
-
- Teter CJ, McCabe SE, Boyd CJ, et al. Illicit methylphenidate use in an undergraduate student sample: prevalence and risk factors. Pharmacotherapy. 2003;23:609–17. - PubMed
-
- Barrett SP, Darredeau C, Bordy LE, et al. Characteristics of methylphenidate misuse in a university student sample. Can J Psychiatry. 2005;50:457–61. - PubMed
-
- Barrett SP, Darredeau C, Pihl RO. Patterns of simultaneous polysubstance use in drug using university students. Hum Psychopharmacol. 2006;21:255–263. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
