

Effects of repeated abobotulinumtoxinA injections in upper limb spasticity
- PMID: 28590525
- PMCID: PMC5811783
- DOI: 10.1002/mus.25721
Effects of repeated abobotulinumtoxinA injections in upper limb spasticity
Abstract
Introduction: The efficacy of single injections of abobotulinumtoxinA (Dysport) is established in adults with upper limb spasticity. In this study we assessed the effects of repeated injections of abobotulinumtoxinA over 1 year.
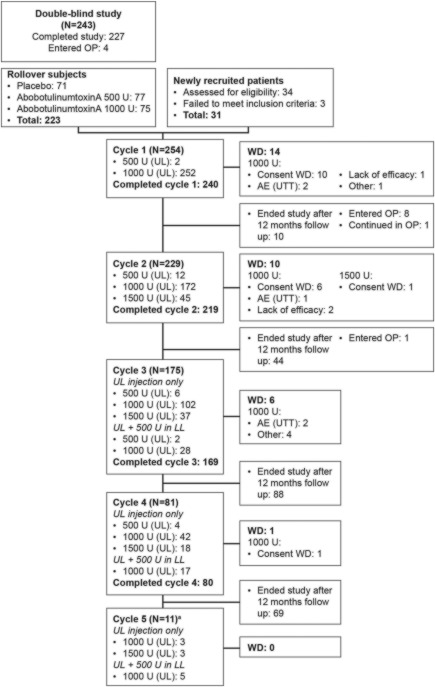
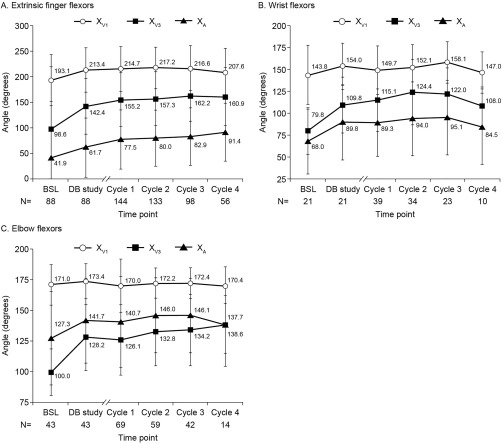
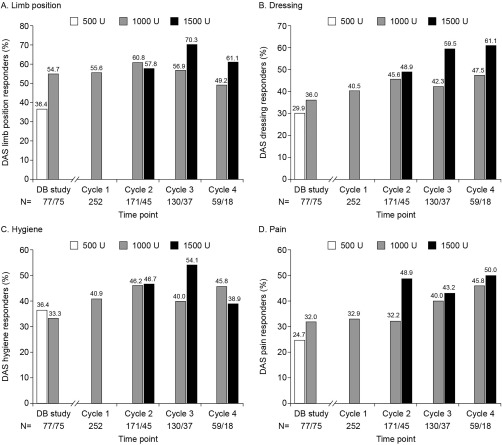
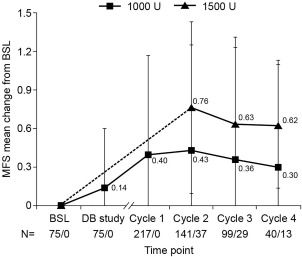
Methods: Patients (n = 258, safety population) received 500 U, 1,000 U, or 1,500 U (1,500-U dose included 500-U shoulder injections) for up to 4 or 5 treatment cycles. Assessments included treatment-emergent adverse events (TEAEs), muscle tone, passive and active range of motion (XV1, XA ), angle of catch (XV3 ), Disability Assessment Scale (DAS) score, Modified Frenchay Scale (MFS) score, and Physician Global Assessment (PGA) score.
Results: The incidence of TEAEs decreased across cycles. Muscle tone reduction and XV1 remained stable across cycles, whereas XV3 and XA continued to improve at the finger, wrist, and elbow flexors. DAS and PGA improved across cycles. MFS improved best with 1,500 U.
Discussion: A favorable safety profile and continuous improvements in active movements and perceived and active function were associated with repeated abobotulinumtoxinA injections in upper limb muscles. Muscle Nerve 57: 245-254, 2018.
Keywords: active function; botulinum toxin; open label; stroke; traumatic brain injury; upper limb spasticity.
© 2017 The Authors Muscle & Nerve Published by Wiley Periodicals, Inc.
Figures
References
-
- Gracies JM. Pathophysiology of spastic paresis. I: Paresis and soft tissue changes. Muscle Nerve 2005;31:535–551. - PubMed
-
- Gracies JM. Pathophysiology of spastic paresis. II: Emergence of muscle overactivity. Muscle Nerve 2005;31:552–571. - PubMed
-
- Sheean G, Lannin NA, Turner‐Stokes L, Rawicki B, Snow BJ, Cerebral Palsy Institute. Botulinum toxin assessment, intervention and after‐care for upper limb hypertonicity in adults: international consensus statement. Eur J Neurol 2010;17(suppl 2):74–93. - PubMed
-
- Wissel J, Ward AB, Erztgaard P, Bensmail D, Hecht MJ, Lejeune TM, et al European consensus table on the use of botulinum toxin type A in adult spasticity. J Rehabil Med 2009;41:13–25. - PubMed
-
- Simpson DM, Hallett M, Ashman EJ, Comella CL, Green MW, Gronseth GS, et al Practice guideline update summary: botulinum neurotoxin for the treatment of blepharospasm, cervical dystonia, adult spasticity, and headache: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 2016;86:1818–1826. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
