

Different surgical approaches for the treatment of adjacent segment diseases after anterior cervical fusion: A retrospective study of 49 patients
- PMID: 28591037
- PMCID: PMC5466215
- DOI: 10.1097/MD.0000000000007042
Different surgical approaches for the treatment of adjacent segment diseases after anterior cervical fusion: A retrospective study of 49 patients
Abstract
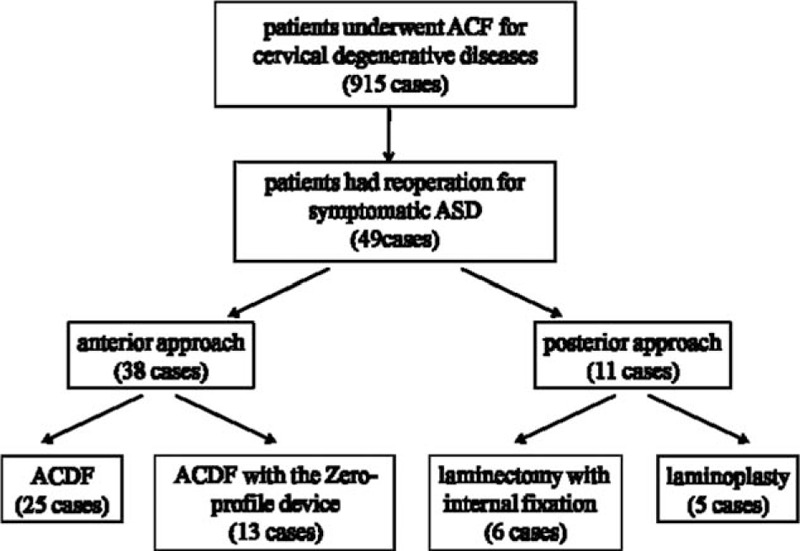
Studies in the literature have not delineated the surgical approaches of symptomatic adjacent segment diseases (ASDs) in patients undergoing reoperation after an initial anterior cervical fusion (ACF). The purpose of this study was to determine the optimal surgical approaches of ASD and the incidence of the dysphagia after reoperation.This was a retrospective study of 49 patients with ASD after an initial ACF surgery, which had undergone a reoperation at our medical center between January 2010 and December 2014. The surgical approaches were used by anterior cervical discectomy and fusion (ACDF), ACDF with the Zero-profile device, laminoplasty, and laminectomy with internal fixation. Patients were classified according to the different surgical approaches of anterior (n = 38) versus posterior (n = 11) groups and ACDF (n = 25) versus Zero-P (n = 13) groups. Clinical evaluations were performed preoperatively and repeated in 24 months after operation.This retrospective study included 26 men and 23 women with a mean age at revision surgery of 54.3 years and ASD onset time of 7.3 years. The patients were followed up with an average of 4.1 years. The reoperation rate was 5.4% in this study. The Japanese Orthopaedic Association (JOA), Neck Disability Index (NDI), and visual analogue scale (VAS) scores demonstrated significant improvements compared with preoperative in both anterior and posterior groups (P < .05). However, there were no differences between the 2 groups (P > .05). The operation time of ACDF group was more than Zero-P group, with significant differences (P < .05). However, there were no differences in JOA, NDI, and VAS scores between the ACDF and Zero-P groups pre- and postoperative (P > .05). A total of 12 (24.5%) patients had dysphagia after reoperation. The incidence of dysphagia in Zero-P group (1/13) was less than ACDF group (11/25), with significant differences (P < .05). There were no cases of major neurological or vascular complications, and wound complications.The clinical situation, initial operation, and secondary preoperative imaging findings were analyzed comprehensively, anterior or posterior approach were chosen, which can effectively relieve spinal cord compression and improve spinal cord function. In ACDF with the Zero-profile device surgery, there was no need to remove the previous internal fixation, shorten the operation time, and reduce the incidence of postoperative dysphagia.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
Similar articles
-
Symptomatic adjacent segment disease after single-lever anterior cervical discectomy and fusion: Incidence and risk factors.Medicine (Baltimore). 2017 Nov;96(47):e8663. doi: 10.1097/MD.0000000000008663. Medicine (Baltimore). 2017. PMID: 29381941 Free PMC article.
-
Is cervical disc arthroplasty good for congenital cervical stenosis?J Neurosurg Spine. 2017 May;26(5):577-585. doi: 10.3171/2016.10.SPINE16317. Epub 2017 Mar 10. J Neurosurg Spine. 2017. PMID: 28291414
-
Comparison of Zero-profile Device Versus Plate-and-Cage Implant in the Treatment of Symptomatic Adjacent Segment Disease after Anterior Cervical Discectomy and Fusion: A Minimum 2-Year Follow-Up Study.World Neurosurg. 2018 Jul;115:e226-e232. doi: 10.1016/j.wneu.2018.04.019. Epub 2018 Apr 12. World Neurosurg. 2018. PMID: 29654956
-
Clinical and Radiographic Outcomes for Patients with Cervical Adjacent Segment Disease Treated with Anterior Cervical Discectomy and Fusion with Integrated Interbody Spacers.World Neurosurg. 2023 Dec;180:e514-e522. doi: 10.1016/j.wneu.2023.09.101. Epub 2023 Sep 28. World Neurosurg. 2023. PMID: 37774788 Review.
-
Anterior cervical discectomy and fusion (ACDF) versus cervical disc arthroplasty (CDA) for two contiguous levels cervical disc degenerative disease: a meta-analysis of randomized controlled trials.Eur Spine J. 2017 Apr;26(4):985-997. doi: 10.1007/s00586-016-4655-5. Epub 2016 Jun 17. Eur Spine J. 2017. PMID: 27314663 Review.
Cited by
-
Risk factors and treatment strategies for adjacent segment disease following spinal fusion (Review).Mol Med Rep. 2025 Feb;31(2):33. doi: 10.3892/mmr.2024.13398. Epub 2024 Nov 22. Mol Med Rep. 2025. PMID: 39575466 Free PMC article. Review.
-
Feasibility of Posterior Cervical Foraminotomy for Adjacent Segmental Disease after Anterior Cervical Fusion.J Korean Neurosurg Soc. 2020 Nov;63(6):767-776. doi: 10.3340/jkns.2020.0033. Epub 2020 Sep 9. J Korean Neurosurg Soc. 2020. PMID: 32898966 Free PMC article.
-
Biomechanical Evaluation of Different Surgical Approaches for the Treatment of Adjacent Segment Diseases After Primary Anterior Cervical Discectomy and Fusion: A Finite Element Analysis.Front Bioeng Biotechnol. 2021 Aug 31;9:718996. doi: 10.3389/fbioe.2021.718996. eCollection 2021. Front Bioeng Biotechnol. 2021. PMID: 34532313 Free PMC article.
-
Symptomatic adjacent segment disease after single-lever anterior cervical discectomy and fusion: Incidence and risk factors.Medicine (Baltimore). 2017 Nov;96(47):e8663. doi: 10.1097/MD.0000000000008663. Medicine (Baltimore). 2017. PMID: 29381941 Free PMC article.
-
Stand-Alone Anchored Spacer vs Anterior Plate Construct in the Management of Adjacent Segment Disease after Anterior Cervical Discectomy and Fusion: A Systematic Review and Meta-Analysis of Comparative Studies.Global Spine J. 2024 Apr;14(3):1038-1051. doi: 10.1177/21925682231201787. Epub 2023 Sep 13. Global Spine J. 2024. PMID: 37705344 Free PMC article. Review.
References
-
- Bohlman HH, Emery SE, Goodfellow DB, et al. Robinson anterior cervical discectomy and arthrodesis for cervical radiculopathy. Long-term follow-up of one hundred and twenty-two patients. J Bone Joint Surg Am 1993;75:1298–307. - PubMed
-
- Gore DR, Sepic SB. Anterior discectomy and fusion for painful cervical disc disease. A report of 50 patients with an average follow-up of 21 years. Spine (Phila Pa 1976) 1998;23:2047–51. - PubMed
-
- Kretzer RM, Hsu W, Hu N, et al. Adjacent-level range of motion and intradiscal pressure after posterior cervical decompression and fixation: an in vitro human cadaveric model. Spine (Phila Pa 1976) 2012;37:E778–785. - PubMed
-
- Shin DA, Yi S, Yoon DH, et al. Artificial disc replacement combined with fusion versus two-level fusion in cervical two-level disc disease. Spine (Phila Pa 1976) 2009;34:1153–9. - PubMed
-
- Lopez-Espina CG, Amirouche F, Havalad V. Multilevel cervical fusion and its effect on disc degeneration and osteophyte formation. Spine (Phila Pa 1976) 2006;31:972–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
