

Perinatal outcomes and congenital heart defect prognosis in 53313 non-selected perinatal infants
- PMID: 28591192
- PMCID: PMC5462529
- DOI: 10.1371/journal.pone.0177229
Perinatal outcomes and congenital heart defect prognosis in 53313 non-selected perinatal infants
Abstract
Objective: To evaluate perinatal outcomes and congenital heart defect (CHD) prognosis in a non-selected population.
Methods: The population-based surveillance data used in this assessment of CHDs were based on birth defect surveillance data collected from 2010-2012 in Liuyang City, China. Infants living with CHDs were followed up for 5 years to determine their prognosis. Prevalence, prenatal diagnosis, perinatal outcomes, and total and type-specific prognosis data were assessed using SPSS 18.0.
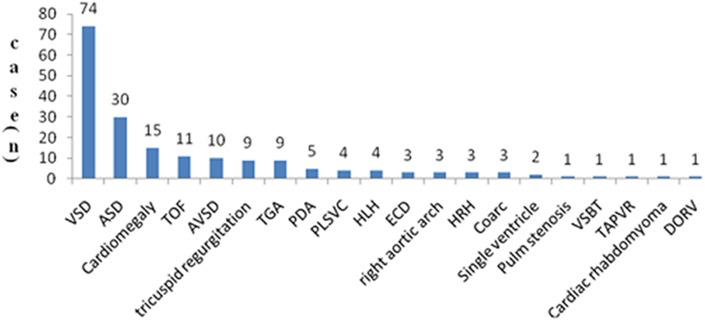
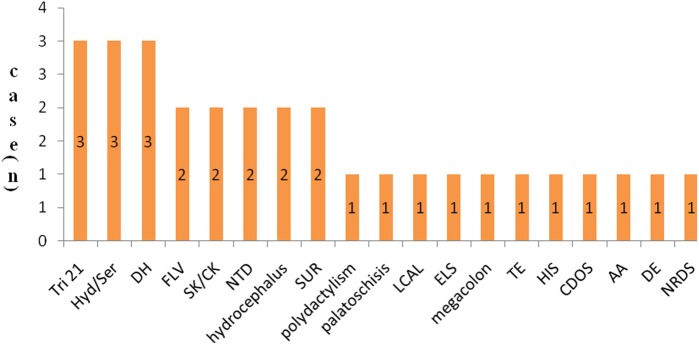
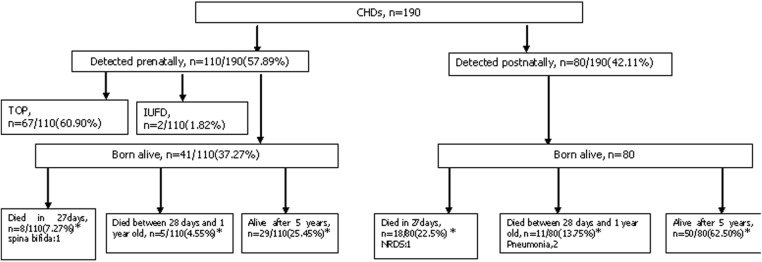
Results: In total, 190 CHD cases were identified among the 53313 included perinatal infants (PIs), indicating a CHD prevalence of 35.64 per 10000 PIs in this non-selected population. The five most frequently identified types of CHDs were ventricular septal defects (VSDs, 38.95%), atrial septal defects (ASDs, 15.79%), cardiomegaly (7.89%), tetralogy of Fallot (TOF, 5.79%), and atrioventricular septal defects (AVSDs, 5.26%). Of the 190 CHD cases, 110 (57.89%) were diagnosed prenatally, 30 (15.79%) were diagnosed with associated malformations, and 69 (36.32%) resulted in termination of pregnancy (TOP). Moreover, 15 (7.89%) PIs died within 7 days after delivery, and 42 (22.10%) died within 1 year. In contrast, 79 (41.58%) were still alive after 5 years. When TOP cases were included, the 5-year survival rate of PIs with prenatally detected CHDs was lower than that of PIs with postnatally detected CHDs (25.45% vs. 63.75%). The CHD subtype associated with the highest rate of infant (less than 1 year old) mortality was transposition of the great arteries (100%). The subtypes associated with higher 5-year survival rates were patent ductus arteriosus (80%), ASD (63.33%), VSD (52.70%) and AVSD (50%).
Conclusions: The rates of prenatal CHD detection and TOP were high in this study population, and the 5-year survival rate of PIs with CHDs was low. The government should strengthen efforts to educate pediatricians regarding this issue and provide financial assistance to improve the prognosis of infants living with CHDs, especially during the first year of life.
Conflict of interest statement
Figures
Similar articles
-
Epidemiology and major subtypes of congenital heart defects in Hunan Province, China.Medicine (Baltimore). 2018 Aug;97(31):e11770. doi: 10.1097/MD.0000000000011770. Medicine (Baltimore). 2018. PMID: 30075604 Free PMC article.
-
Survival analysis of Down syndrome with congenital heart disease: a 5-years registry at QSNICH.J Med Assoc Thai. 2014 Jun;97 Suppl 6:S108-14. J Med Assoc Thai. 2014. PMID: 25391181
-
Epidemiology of Congenital Heart Defects in Perinatal Infants in Guangxi, China.Int J Gen Med. 2024 Nov 18;17:5381-5396. doi: 10.2147/IJGM.S466195. eCollection 2024. Int J Gen Med. 2024. PMID: 39582917 Free PMC article.
-
Prevalence, treatment, and outcome of heart disease in live-born children: a prospective analysis of 91,823 live-born children.Pediatr Cardiol. 1989 Fall;10(4):205-11. doi: 10.1007/BF02083294. Pediatr Cardiol. 1989. PMID: 2687820 Review.
-
Congenital heart disease in adults.Cardiovasc Clin. 1970;2(1):257-65. Cardiovasc Clin. 1970. PMID: 4938799 Review. No abstract available.
Cited by
-
Genetic and Clinical Features of Heterotaxy in a Prenatal Cohort.Front Genet. 2022 Apr 19;13:818241. doi: 10.3389/fgene.2022.818241. eCollection 2022. Front Genet. 2022. PMID: 35518361 Free PMC article.
-
A novel stop-gain pathogenic variant in FLT4 and a nonsynonymous pathogenic variant in PTPN11 associated with congenital heart defects.Eur J Med Res. 2022 Dec 10;27(1):286. doi: 10.1186/s40001-022-00920-8. Eur J Med Res. 2022. PMID: 36496429 Free PMC article.
-
Non-Coding RNAs as Blood-Based Biomarkers in Cardiovascular Disease.Int J Mol Sci. 2020 Dec 5;21(23):9285. doi: 10.3390/ijms21239285. Int J Mol Sci. 2020. PMID: 33291434 Free PMC article. Review.
-
Impacts of prenatal diagnosis of congenital heart diseases on outcomes.Transl Pediatr. 2021 Aug;10(8):2241-2249. doi: 10.21037/tp-20-267. Transl Pediatr. 2021. PMID: 34584895 Free PMC article. Review.
-
Prevalence and death rate of birth defects from population-based surveillance in Hunan Province, China, 2010-2020.Sci Rep. 2024 Jun 25;14(1):14609. doi: 10.1038/s41598-024-65072-7. Sci Rep. 2024. PMID: 38918397 Free PMC article.
References
-
- Olney R. S., Ailes E. C. and Sontag M. K. Detection of critical congenital heart defects: Review of contributions from prenatal and newborn screening. Semin Perinatol. 2015; 39(3): 230–237. doi: 10.1053/j.semperi.2015.03.007 - DOI - PMC - PubMed
-
- Talner C. N. Report of the new england regional infant cardiac program, by donald c. Fyler, md, pediatrics, 1980;65(suppl):375–461. Pediatrics. 1998; 102(1 Pt 2): 258–259. - PubMed
-
- Pradat P., Francannet C., Harris J. A. and Robert E. The epidemiology of cardiovascular defects, part i: A study based on data from three large registries of congenital malformations. Pediatr Cardiol. 2003; 24(3): 195–221. doi: 10.1007/s00246-002-9401-6 - DOI - PubMed
-
- Hoffman J. I. and Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol. 2002; 39(12): 1890–1900. - PubMed
-
- Report of the new england regional infant cardiac program. Pediatrics. 1980; 65(2 Pt 2): 375–461. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
