

Different strategies for mechanical VENTilation during CardioPulmonary Bypass (CPBVENT 2014): study protocol for a randomized controlled trial
- PMID: 28592276
- PMCID: PMC5463370
- DOI: 10.1186/s13063-017-2008-2
Different strategies for mechanical VENTilation during CardioPulmonary Bypass (CPBVENT 2014): study protocol for a randomized controlled trial
Abstract
Background: There is no consensus on which lung-protective strategies should be used in cardiac surgery patients. Sparse and small randomized clinical and animal trials suggest that maintaining mechanical ventilation during cardiopulmonary bypass is protective on the lungs. Unfortunately, such evidence is weak as it comes from surrogate and minor clinical endpoints mainly limited to elective coronary surgery. According to the available data in the academic literature, an unquestionable standardized strategy of lung protection during cardiopulmonary bypass cannot be recommended. The purpose of the CPBVENT study is to investigate the effectiveness of different strategies of mechanical ventilation during cardiopulmonary bypass on postoperative pulmonary function and complications.
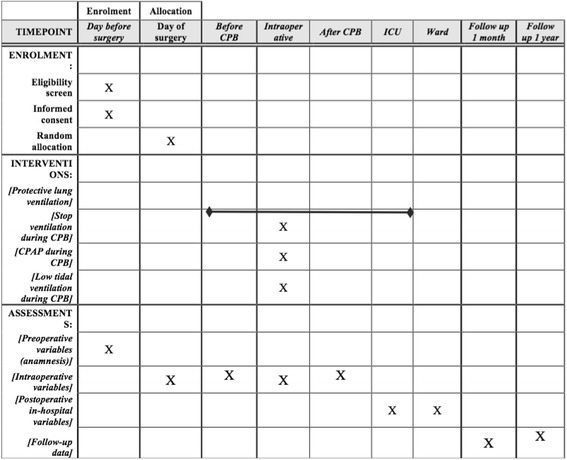
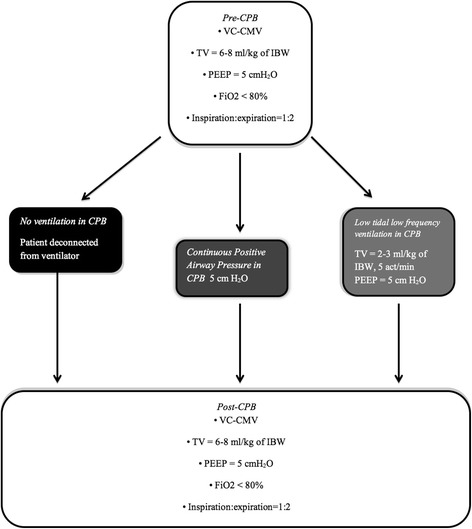
Methods/design: The CPBVENT study is a single-blind, multicenter, randomized controlled trial. We are going to enroll 870 patients undergoing elective cardiac surgery with planned use of cardiopulmonary bypass. Patients will be randomized into three groups: (1) no mechanical ventilation during cardiopulmonary bypass, (2) continuous positive airway pressure of 5 cmH2O during cardiopulmonary bypass, (3) respiratory rate of 5 acts/min with a tidal volume of 2-3 ml/Kg of ideal body weight and positive end-expiratory pressure of 3-5 cmH2O during cardiopulmonary bypass. The primary endpoint will be the incidence of a PaO2/FiO2 ratio <200 until the time of discharge from the intensive care unit. The secondary endpoints will be the incidence of postoperative pulmonary complications and 30-day mortality. Patients will be followed-up for 12 months after the date of randomization.
Discussion: The CPBVENT trial will establish whether, and how, different ventilator strategies during cardiopulmonary bypass will have an impact on postoperative pulmonary complications and outcomes of patients undergoing cardiac surgery.
Trial registration: ClinicalTrials.gov, ID: NCT02090205 . Registered on 8 March 2014.
Keywords: CPAP; Cardiopulmonary bypass; Low tidal volume; Postoperative pulmonary complications; Protective ventilation; Respiratory insufficiency; Systemic inflammatory response.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
