

Dabrafenib plus trametinib in patients with BRAFV600-mutant melanoma brain metastases (COMBI-MB): a multicentre, multicohort, open-label, phase 2 trial
- PMID: 28592387
- PMCID: PMC5991615
- DOI: 10.1016/S1470-2045(17)30429-1
Dabrafenib plus trametinib in patients with BRAFV600-mutant melanoma brain metastases (COMBI-MB): a multicentre, multicohort, open-label, phase 2 trial
Abstract
Background: Dabrafenib plus trametinib improves clinical outcomes in BRAFV600-mutant metastatic melanoma without brain metastases; however, the activity of dabrafenib plus trametinib has not been studied in active melanoma brain metastases. Here, we report results from the phase 2 COMBI-MB trial. Our aim was to build on the current body of evidence of targeted therapy in melanoma brain metastases through an evaluation of dabrafenib plus trametinib in patients with BRAFV600-mutant melanoma brain metastases.
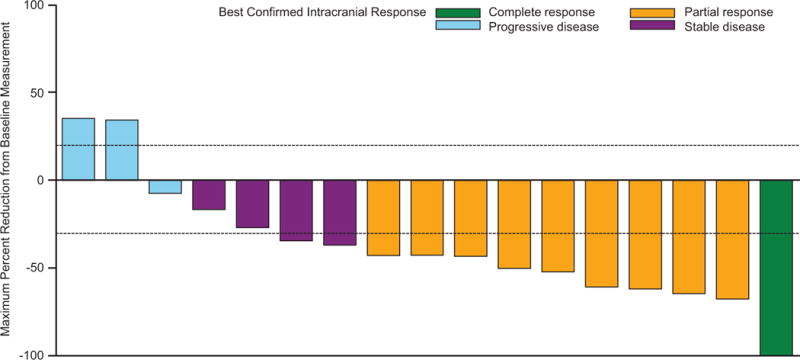
Methods: This ongoing, multicentre, multicohort, open-label, phase 2 study evaluated oral dabrafenib (150 mg twice per day) plus oral trametinib (2 mg once per day) in four patient cohorts with melanoma brain metastases enrolled from 32 hospitals and institutions in Europe, North America, and Australia: (A) BRAFV600E-positive, asymptomatic melanoma brain metastases, with no previous local brain therapy, and an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1; (B) BRAFV600E-positive, asymptomatic melanoma brain metastases, with previous local brain therapy, and an ECOG performance status of 0 or 1; (C) BRAFV600D/K/R-positive, asymptomatic melanoma brain metastases, with or without previous local brain therapy, and an ECOG performance status of 0 or 1; and (D) BRAFV600D/E/K/R-positive, symptomatic melanoma brain metastases, with or without previous local brain therapy, and an ECOG performance status of 0, 1, or 2. The primary endpoint was investigator-assessed intracranial response in cohort A in the all-treated-patients population. Secondary endpoints included intracranial response in cohorts B, C, and D. This study is registered with ClinicalTrials.gov, number NCT02039947.
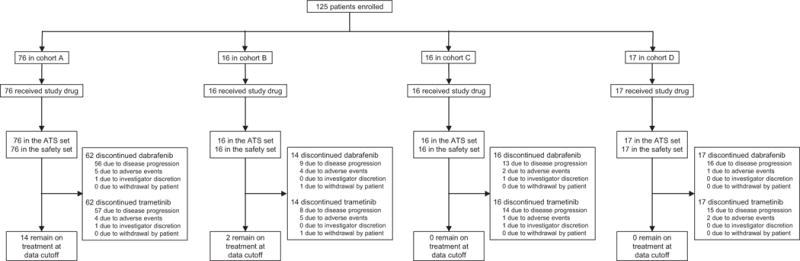
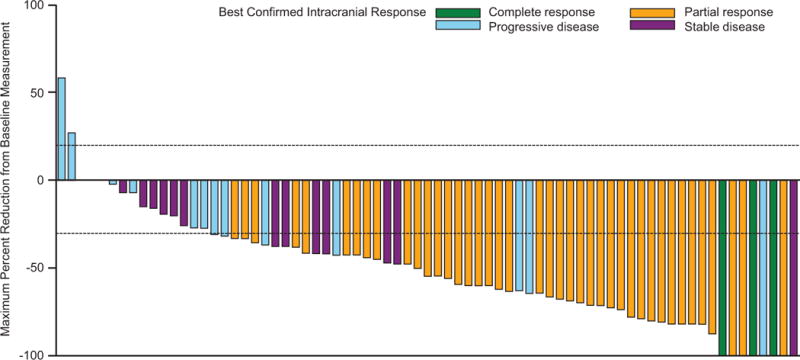
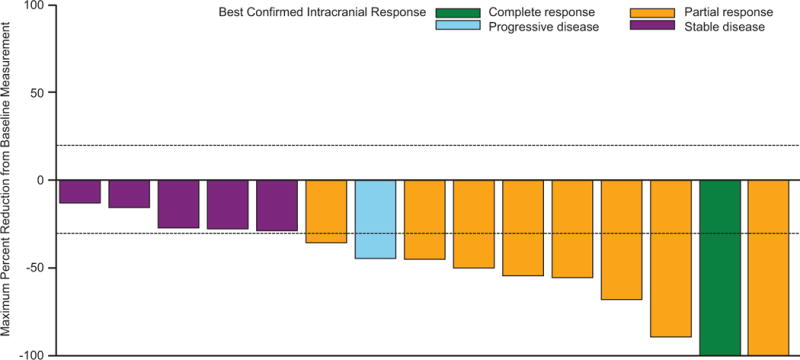
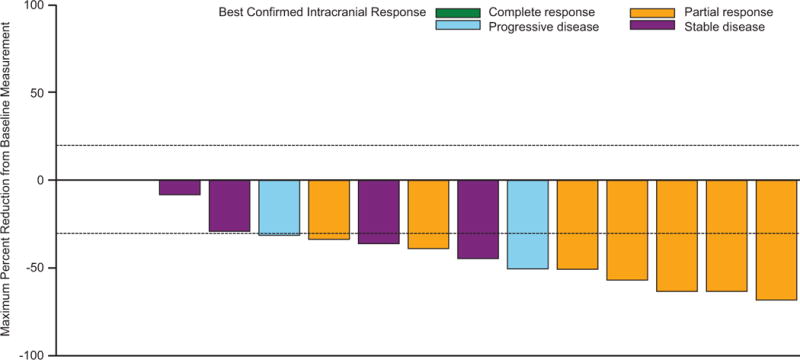
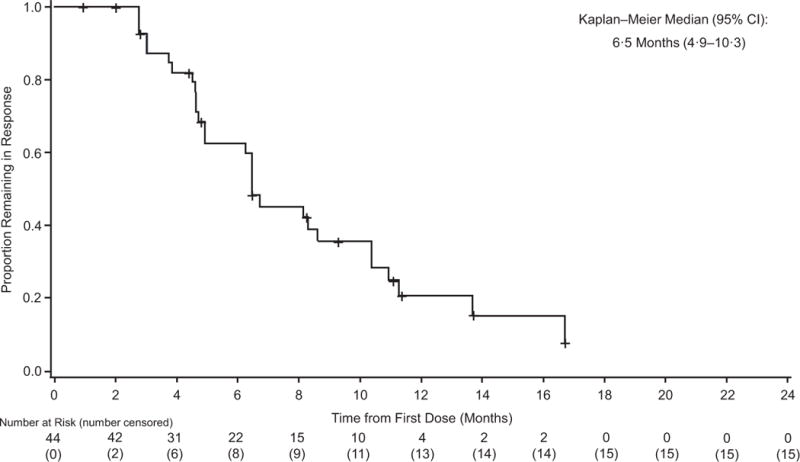
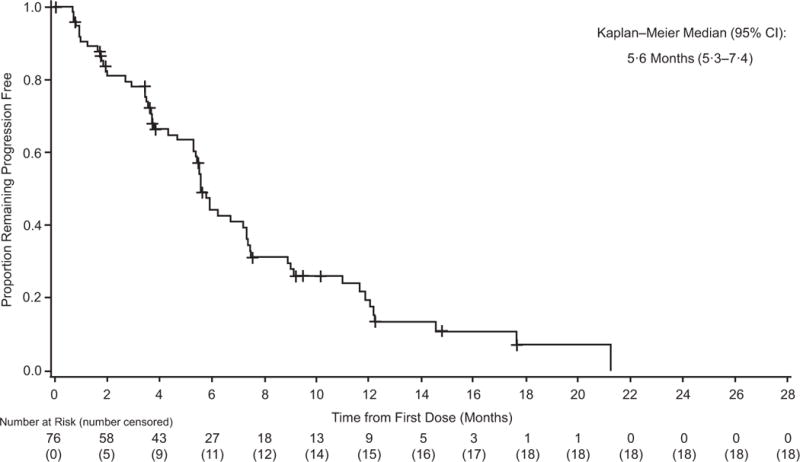
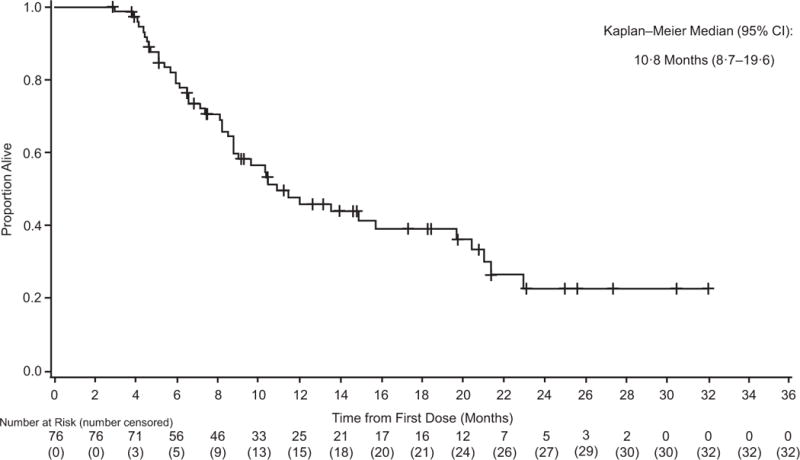
Findings: Between Feb 28, 2014, and Aug 5, 2016, 125 patients were enrolled in the study: 76 patients in cohort A; 16 patients in cohort B; 16 patients in cohort C; and 17 patients in cohort D. At the data cutoff (Nov 28, 2016) after a median follow-up of 8·5 months (IQR 5·5-14·0), 44 (58%; 95% CI 46-69) of 76 patients in cohort A achieved an intracranial response. Intracranial response by investigator assessment was also achieved in nine (56%; 95% CI 30-80) of 16 patients in cohort B, seven (44%; 20-70) of 16 patients in cohort C, and ten (59%; 33-82) of 17 patients in cohort D. The most common serious adverse events related to study treatment were pyrexia for dabrafenib (eight [6%] of 125 patients) and decreased ejection fraction (five [4%]) for trametinib. The most common grade 3 or worse adverse events, regardless of study drug relationship, were pyrexia (four [3%] of 125) and headache (three [2%]).
Interpretation: Dabrafenib plus trametinib was active with a manageable safety profile in this melanoma population that was consistent with previous dabrafenib plus trametinib studies in patients with BRAFV600-mutant melanoma without brain metastases, but the median duration of response was relatively short. These results provide evidence of clinical benefit with dabrafenib plus trametinib and support the need for additional research to further improve outcomes in patients with melanoma brain metastases.
Funding: Novartis.
Copyright © 2017 Elsevier Ltd. All rights reserved.
Conflict of interest statement
MAD has been a principal investigator grants to his institution received from AstraZeneca, Merck, Roche/Genentech, and Sanofi; and has received personal fees from Novartis, Bristol-Myers Squibb, Sanofi, and Merck for advisory board participation. PS has received personal fees from Amgen, Bristol-Myers Squibb, MSD, Merck-Serono, Pfizer, Roche/Genentech, Pierre Fabre, and Novartis; has received nonfinancial support from Bristol-Myers Squibb, MSD, Roche/Genentech, and Novartis; and has received funding grant from Roche/Genentech. CR has received personal fees for advisory board participation from Bristol-Myers Squibb, GlaxoSmithKline, Roche, Merck, Amgen, and Novartis. J-JG has received personal fees for participating in advisory boards for Novartis, Roche, GlaxoSmithKline, Bristol-Myers Squibb, Merck, Amgen, and Pierre Fabre. KTF has received personal fees and grant support from Novartis. AA has received personal fees from Novartis, Roche, Merck/MSD, and Bristol-Myers Squibb and financial support for the study from Novartis. VC-S has participated in advisory boards for Merck/MSD, Merck-Serono, Roche, Bristol-Myers Squibb, and Novartis. LT has nothing to disclose. TL has received grants and personal fees for clinical trials and advisory board participation from Bristol-Myers Squibb, Roche, Novartis, and MSD; has participated in speakers’ bureaus for Roche, MSD, and Novartis; and has received travel/accommodations expenses from Roche. LM has nothing to disclose. SJM has received personal fees for consultancy or travel from Merck, Amgen, Novartis and and Bristol-Myers Squibb; and has received grants from Merck, Amgen, and Pharmacyclics. DH has received personal fees for advisory board participation or lectures from Roche, Bristol-Myers Squibb, EMD Serono, Merck, Amgen, and Novartis. IM-R has received personal fees from Novartis, Roche, MSD, Amgen, Merck-Serono, Pierre Fabre, Bioncotech, GlaxoSmithKline, and Bristol-Myers Squibb and has received travel/accommodation expenses from MSD, Bristol-Myers Squibb, and Amgen. MDV has consulted or had an advisory role for and received honoraria from Bristol-Myers Squibb, Roche, Novartis, and Merck. CL has received grants from Roche and Bristol-Myers Squibb and personal fees for consultancy, advisory roles, speaker’s bureaus, and/or travel/accommodation expenses from Roche, Bristol-Myers Squibb, Novartis, Merck/MSD, Amgen, and GlaxoSmithKline. NM has received personal fees from Roche, Bristol-Myers Squibb, MSD, Novartis, GlaxoSmithKline, Pierre Fabre, and grants from Bristol-Myers Squibb, MSD, and Pierre Fabre. YZ, YH, and BM are employees of Novartis. GVL received personal fees for her role as a consultant advisor to Amgen, Bristol-Myers Squibb, Merck/MSD, Novartis, Pierre Fabre, Array Biopharma, and Roche.
Figures
Comment in
-
BRAF-MEK inhibition in melanoma brain metastases: a new hope.Lancet Oncol. 2017 Jul;18(7):836-837. doi: 10.1016/S1470-2045(17)30449-7. Lancet Oncol. 2017. PMID: 28677560 No abstract available.
-
Primary medical therapy for BRAFV600E-mutant melanoma brain metastases-is this good enough?Lancet Oncol. 2017 Sep;18(9):e508. doi: 10.1016/S1470-2045(17)30633-2. Lancet Oncol. 2017. PMID: 28884696 No abstract available.
-
Primary medical therapy for BRAFV600E-mutant melanoma brain metastases-is this good enough? - Authors' reply.Lancet Oncol. 2017 Sep;18(9):e509. doi: 10.1016/S1470-2045(17)30640-X. Lancet Oncol. 2017. PMID: 28884697 No abstract available.
References
-
- Sampson JH, Carter JH, Jr, Friedman AH, Seigler HF. Demographics, prognosis, and therapy in 702 patients with brain metastases from malignant melanoma. J Neurosurg. 1998;88:11–20. - PubMed
-
- Long GV, Margolin KA. Multidisciplinary approach to brain metastasis from melanoma: the emerging role of systemic therapies. Am Soc Clin Oncol Educ Book. 2013:393–8. - PubMed
-
- Davies MA, Liu P, McIntyre S, et al. Prognostic factors for survival in melanoma patients with brain metastases. Cancer. 2011;117:1687–96. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
