

Combined immune checkpoint blockade as a therapeutic strategy for BRCA1-mutated breast cancer
- PMID: 28592566
- PMCID: PMC5822709
- DOI: 10.1126/scitranslmed.aal4922
Combined immune checkpoint blockade as a therapeutic strategy for BRCA1-mutated breast cancer
Abstract
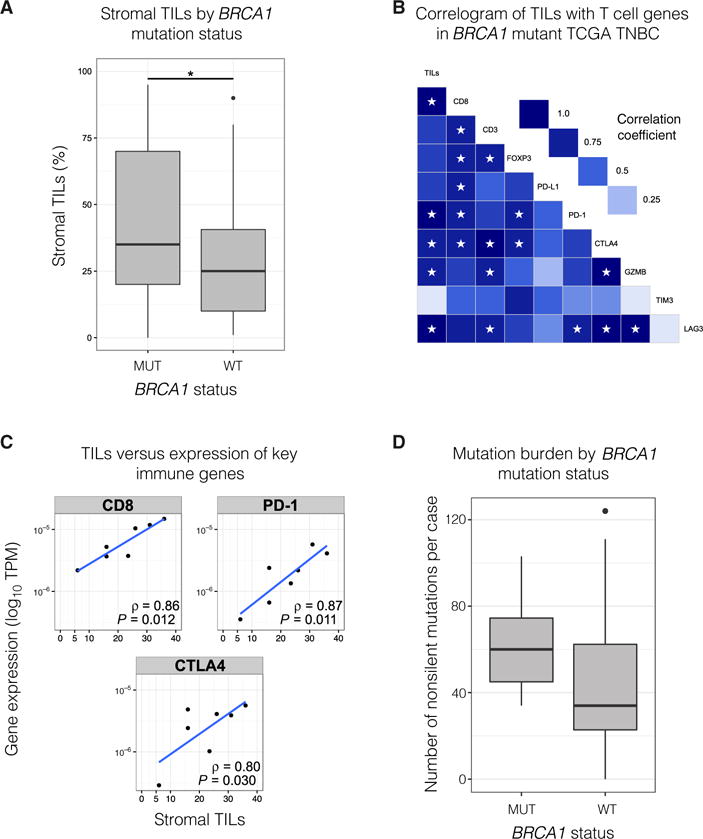
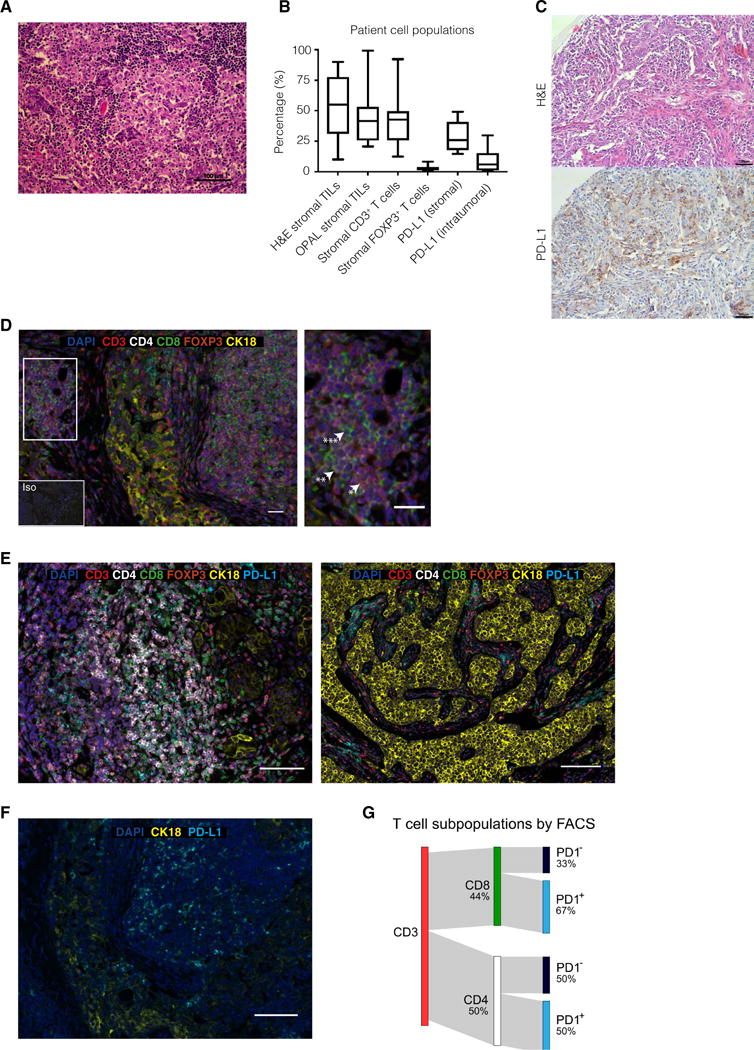
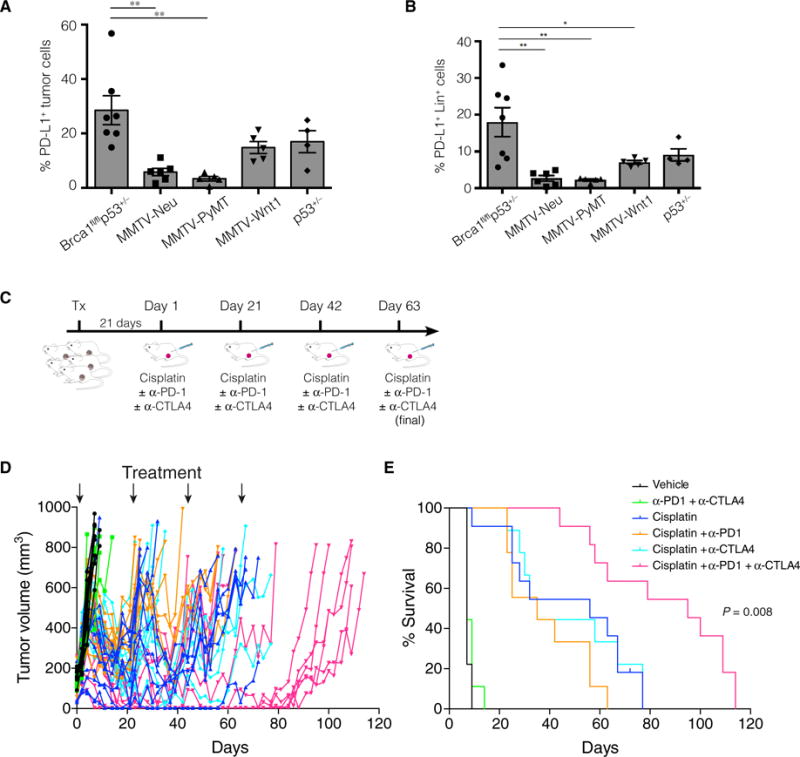
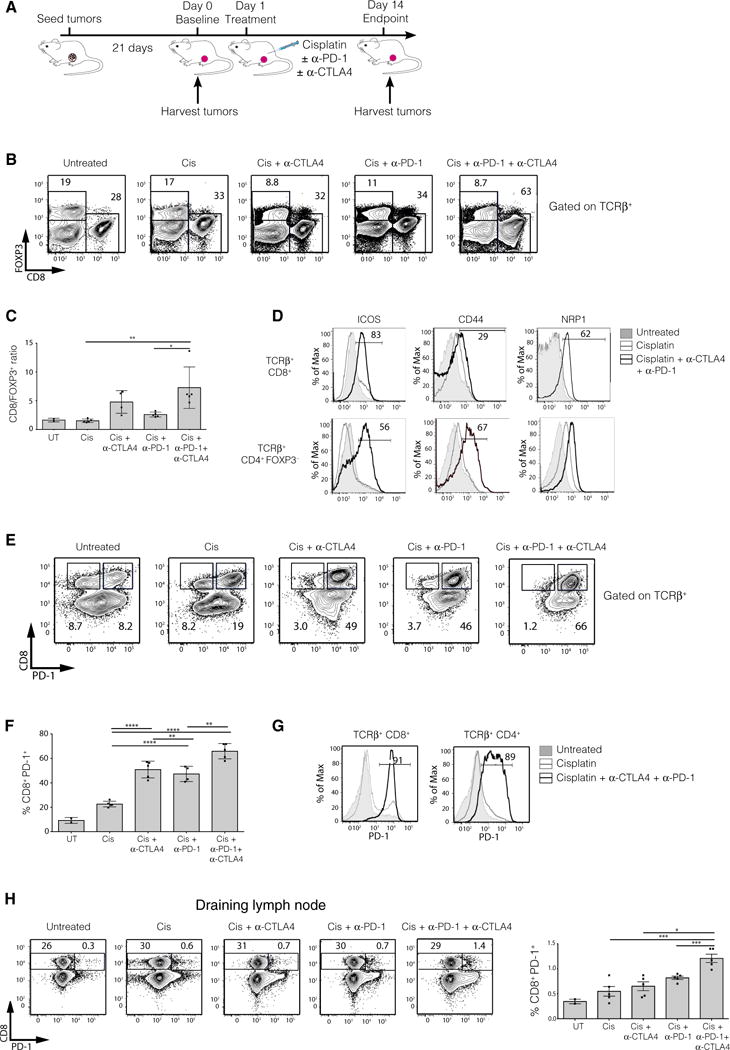
Immune checkpoint inhibitors have emerged as a potent new class of anticancer therapy. They have changed the treatment landscape for a range of tumors, particularly those with a high mutational load. To date, however, modest results have been observed in breast cancer, where tumors are rarely hypermutated. Because BRCA1-associated tumors frequently exhibit a triple-negative phenotype with extensive lymphocyte infiltration, we explored their mutational load, immune profile, and response to checkpoint inhibition in a Brca1-deficient tumor model. BRCA1-mutated triple-negative breast cancers (TNBCs) exhibited an increased somatic mutational load and greater numbers of tumor-infiltrating lymphocytes, with increased expression of immunomodulatory genes including PDCD1 (PD-1) and CTLA4, when compared to TNBCs from BRCA1-wild-type patients. Cisplatin treatment combined with dual anti-programmed death-1 and anti-cytotoxic T lymphocyte-associated antigen 4 therapy substantially augmented antitumor immunity in Brca1-deficient mice, resulting in an avid systemic and intratumoral immune response. This response involved enhanced dendritic cell activation, reduced suppressive FOXP3+ regulatory T cells, and concomitant increase in the activation of tumor-infiltrating cytotoxic CD8+ and CD4+ T cells, characterized by the induction of polyfunctional cytokine-producing T cells. Dual (but not single) checkpoint blockade together with cisplatin profoundly attenuated the growth of Brca1-deficient tumors in vivo and improved survival. These findings provide a rationale for clinical studies of combined immune checkpoint blockade in BRCA1-associated TNBC.
Copyright © 2017, American Association for the Advancement of Science.
Conflict of interest statement
Figures
Comment in
-
Immunotherapy: Keeping breast cancer in check.Nat Rev Cancer. 2017 Aug;17(8):454-455. doi: 10.1038/nrc.2017.55. Epub 2017 Jul 7. Nat Rev Cancer. 2017. PMID: 28684877 No abstract available.
-
Doubling Down on BRCA-Mutated Cancer.Trends Cancer. 2017 Nov;3(11):743-744. doi: 10.1016/j.trecan.2017.09.005. Epub 2017 Sep 29. Trends Cancer. 2017. PMID: 29120748
References
-
- Foulkes WD, Smith IE, Reis-Filho JS. Triple-negative breast cancer. N Engl J Med. 2010;363:1938–1948. - PubMed
-
- Lord CJ, Ashworth A. BRCAness revisited. Nat Rev Cancer. 2016;16:110–120. - PubMed
-
- Bouwman P, Jonkers J. Molecular pathways: How can BRCA-mutated tumors become resistant to PARP inhibitors? Clin Cancer Res. 2014;20:540–547. - PubMed
-
- Schreiber RD, Old LJ, Smyth MJ. Cancer immunoediting: Integrating immunity’s roles in cancer suppression and promotion. Science. 2011;331:1565–1570. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
