

Cholecystokinin responsiveness varies across the population dependent on metabolic phenotype
- PMID: 28592602
- PMCID: PMC5525122
- DOI: 10.3945/ajcn.117.156943
Cholecystokinin responsiveness varies across the population dependent on metabolic phenotype
Abstract
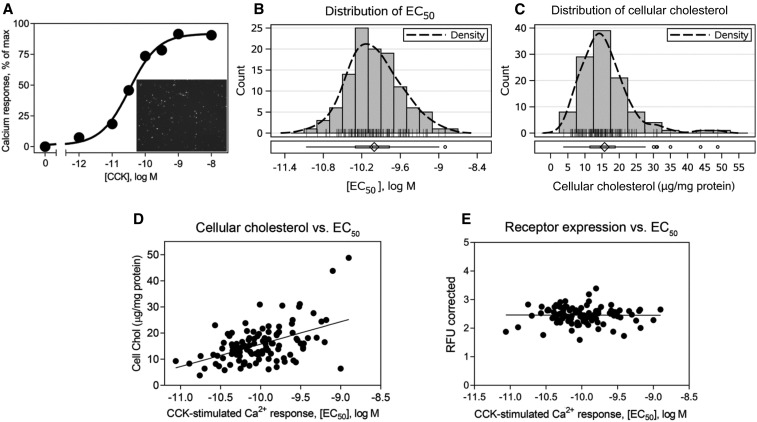
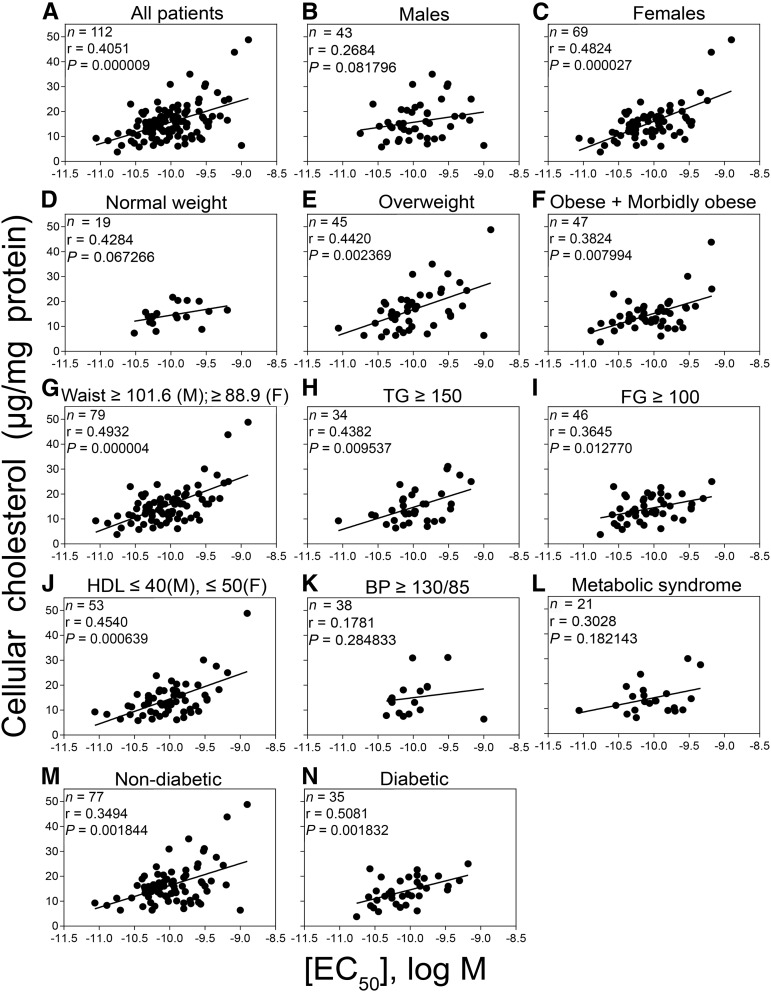
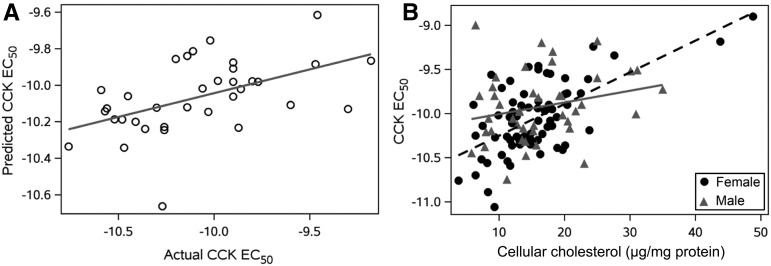
Background: Cholecystokinin (CCK) is an important satiety factor, acting at type 1 receptors (CCK1Rs) on vagal afferent neurons; however, CCK agonists have failed clinical trials for obesity. We postulated that CCK1R function might be defective in such patients due to abnormal membrane composition, such as that observed in cholesterol gallstone disease.Objective: Due to the challenges in directly studying CCK1Rs relevant to appetite control, our goal was to develop and apply a method to determine the impact of a patient's own cellular environment on CCK stimulus-activity coupling and to determine whether CCK sensitivity correlated with the metabolic phenotype of a high-risk population.Design: Wild-type CCK1Rs were expressed on leukocytes from 112 Hispanic patients by using adenoviral transduction and 24-h culture, with quantitation of cholesterol composition and intracellular calcium responses to CCK. Results were correlated with clinical, biochemical, and morphometric characteristics.Results: Broad ranges of cellular cholesterol and CCK responsiveness were observed, with elevated cholesterol correlated with reduced CCK sensitivity. This was prominent with increasing degrees of obesity and the presence of diabetes, particularly when poorly controlled. No single standard clinical metric correlated directly with CCK responsiveness. Reduced CCK sensitivity best correlated with elevated serum triglycerides in normal-weight participants and with low HDL concentrations and elevated glycated hemoglobin in obese and diabetic patients.Conclusions: CCK responsiveness varies widely across the population, with reduced signaling in patients with obesity and diabetes. This could explain the failure of CCK agonists in previous clinical trials and supports the rationale to develop corrective modulators to reverse this defective servomechanism for appetite control. This trial was registered at www.clinicaltrials.gov as NCT03121755.
Keywords: cholecystokinin; cholesterol; epidemiology; hormonal responsiveness; obesity drug development; population study.
© 2017 American Society for Nutrition.
Figures
Comment in
-
Modulation of receptor signaling by metabolic environment.Am J Clin Nutr. 2017 Aug;106(2):437-438. doi: 10.3945/ajcn.117.161554. Epub 2017 Jul 12. Am J Clin Nutr. 2017. PMID: 28701301 Free PMC article. No abstract available.
References
-
- Trevaskis JL, Turek VF, Griffin PS, Wittmer C, Parkes DG, Roth JD. Multi-hormonal weight loss combinations in diet-induced obese rats: therapeutic potential of cholecystokinin? Physiol Behav 2010;100:187–95. - PubMed
-
- Young AA. Brainstem sensing of meal-related signals in energy homeostasis. Neuropharmacology 2012;63:31–45. - PubMed
-
- Pi-Sunyer X, Astrup A, Fujioka K, Greenway F, Halpern A, Krempf M, Lau DC, le Roux CW, Violante Ortiz R, Jensen CB, et al. A randomized, controlled trial of 3.0 mg of liraglutide in weight management. N Engl J Med 2015;373:11–22. - PubMed
-
- Holmes D. Diabetes: concerns about long-term use of GLP-1 analogues. Nat Rev Endocrinol 2016;12:186. - PubMed
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
