

Treatment advances and prognosis for patients with adult T-cell leukemia-lymphoma
- PMID: 28592744
- PMCID: PMC6144188
- DOI: 10.3960/jslrt.17008
Treatment advances and prognosis for patients with adult T-cell leukemia-lymphoma
Abstract
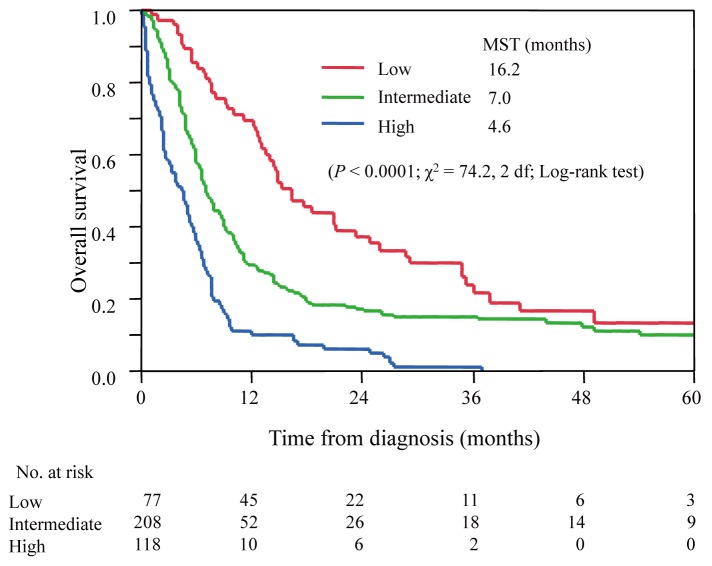
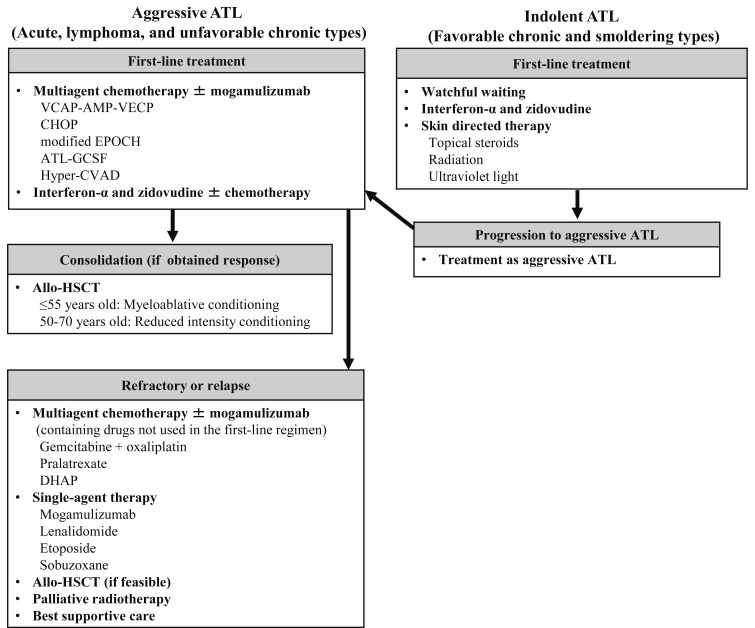
A classification for adult T-cell leukemia-lymphoma (ATL) based on clinical features was proposed in 1991: acute, lymphoma, chronic, and smoldering types, and their median survival times (MSTs) were reported to be 6.2, 10.2, 24.3 months, and not reached, respectively. Several new therapies for ATL have since been developed, i.e. dose-intensity multi-agent chemotherapies, allogeneic hematopoietic stem cell transplantation (allo-HSCT), monoclonal antibodies, and anti-viral therapy. The monoclonal antibody to CCR4, mogamulizumab, clearly improved response rates in patients with treatment-naïve and relapsed aggressive ATL, and has the potential to provide a survival advantage. The outcomes of allo-HSCT have been reported since the early 2000s. High treatment-related mortality was initially the crucial issue associated with this treatment approach; however, reduced intensity conditioning regimens have decreased the risk of treatment-related mortality. The introduction of allo- HSCT has had a positive impact on the prognosis of and potential curability with treatments for ATL. A meta-analysis of a treatment with interferon-α and zidovudine (IFN/AZT) revealed a survival benefit in patients with the leukemic subtype. A phase 3 study comparing IFN/AZT with watchful waiting in patients with indolent ATL is ongoing in Japan. Several clinical trials on novel agents are currently being conducted, such as the histone deacetylase inhibitors, alemtuzumab, brentuximab vedotin, nivolumab, and an EZH1/2 dual inhibitor.
Keywords: adult T-cell leukemia-lymphoma; allogeneic hematopoietic stem cell transplantation; dose-intensity multi-agent chemotherapy.
Conflict of interest statement
K.I. reports grants and personal fees from Kyowa Hakko Kirin, Chugai Pharmaceutical, Takeda Pharmaceutical, Novartis, Eisai, and Taiho Pharmaceutical; personal fees from Bristol-Myers Squibb, Celgene, Janssen Pharmaceutical, and Pfizer; and grants from Yakult Pharmaceutical, MSD, and Japan Blood Products Organization, outside the submitted work.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources