

CT-Based Local Distribution Metric Improves Characterization of COPD
- PMID: 28592874
- PMCID: PMC5462827
- DOI: 10.1038/s41598-017-02871-1
CT-Based Local Distribution Metric Improves Characterization of COPD
Abstract
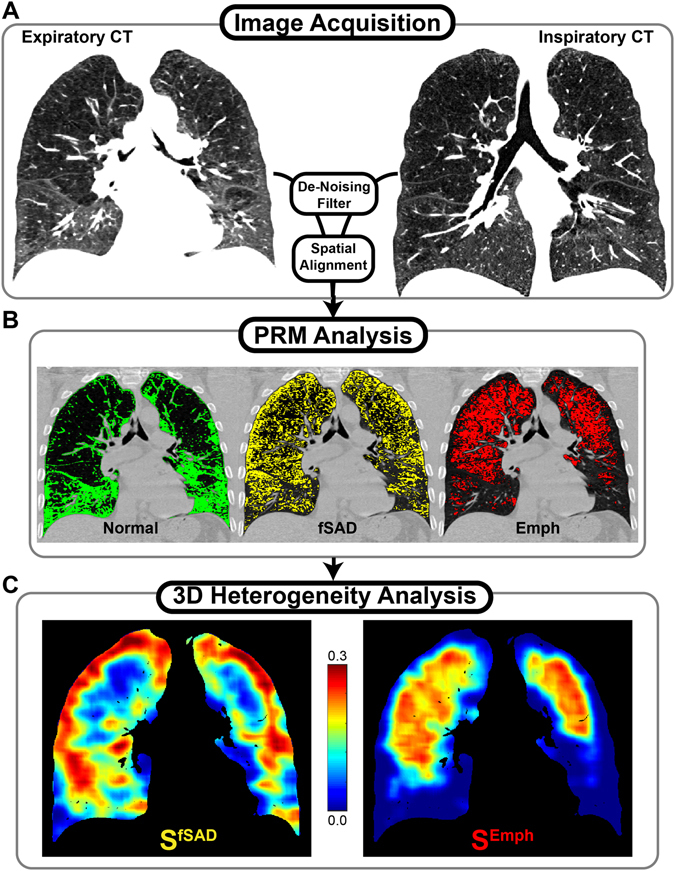
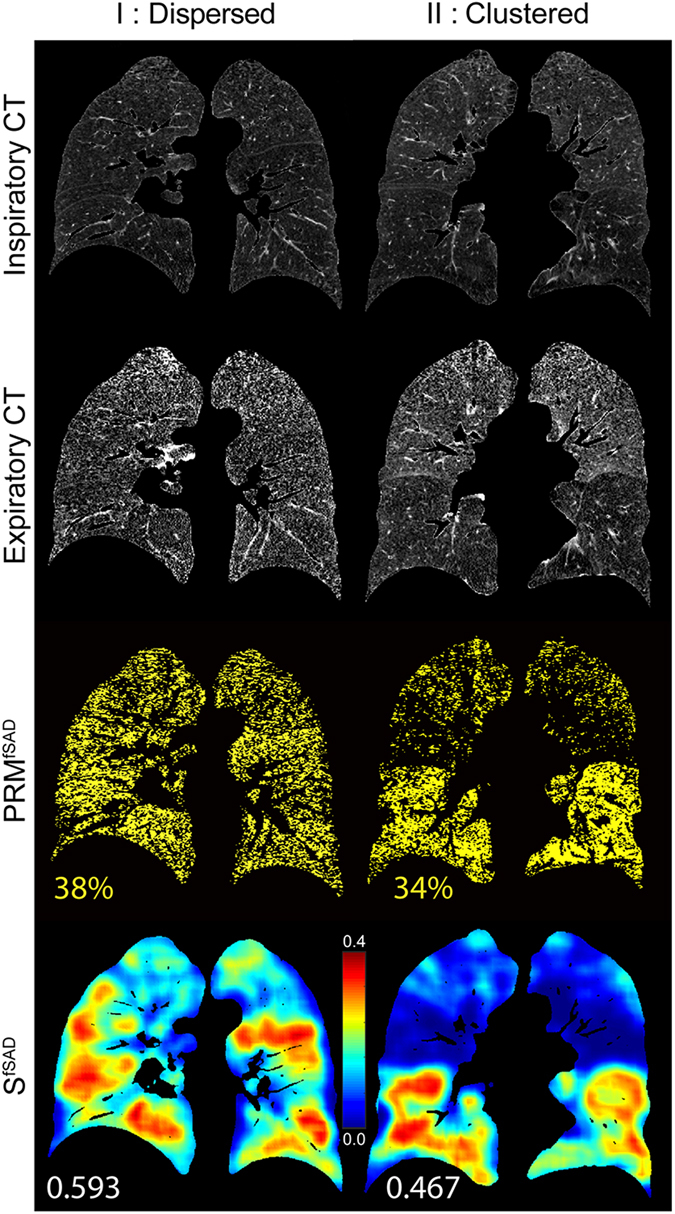
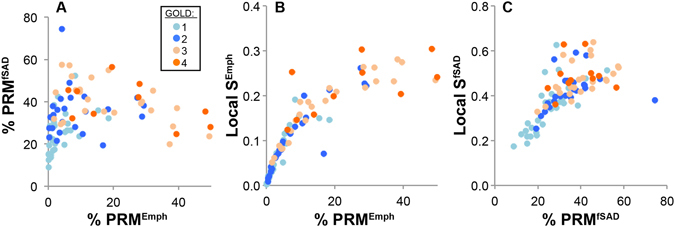
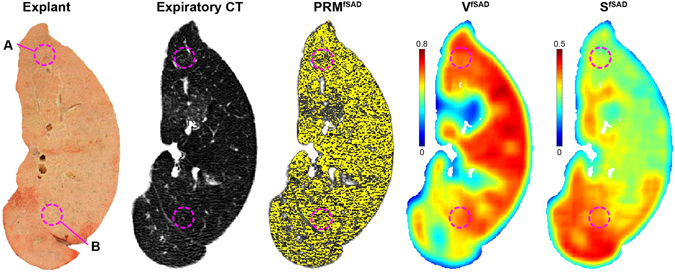
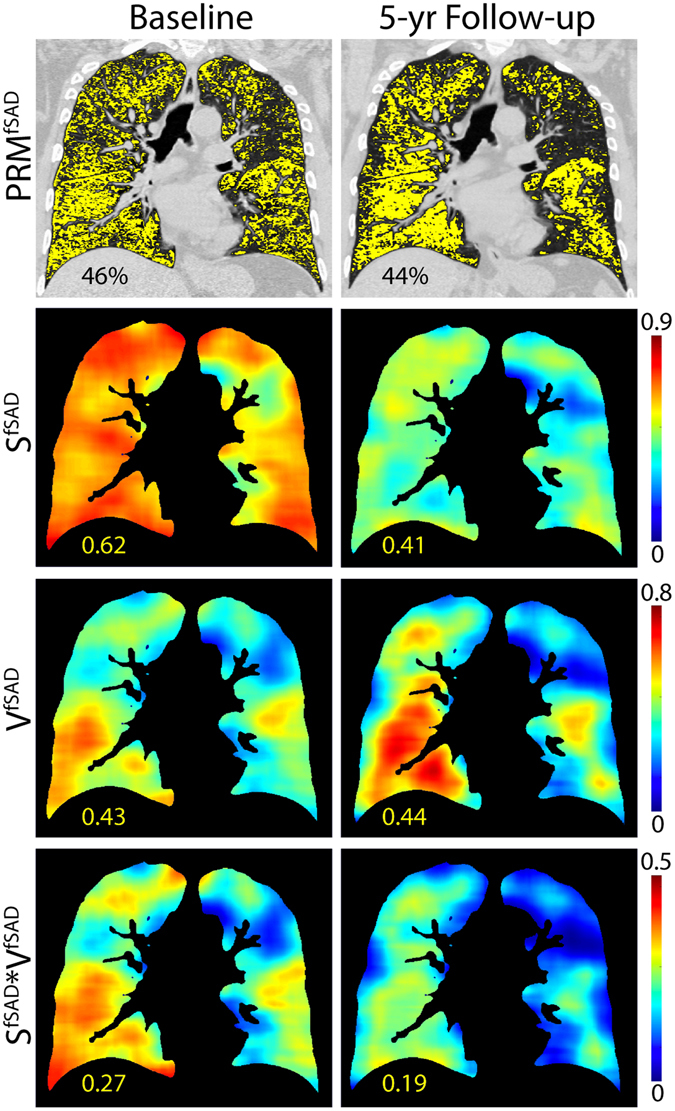
Parametric response mapping (PRM) of paired CT lung images has been shown to improve the phenotyping of COPD by allowing for the visualization and quantification of non-emphysematous air trapping component, referred to as functional small airways disease (fSAD). Although promising, large variability in the standard method for analyzing PRMfSAD has been observed. We postulate that representing the 3D PRMfSAD data as a single scalar quantity (relative volume of PRMfSAD) oversimplifies the original 3D data, limiting its potential to detect the subtle progression of COPD as well as varying subtypes. In this study, we propose a new approach to analyze PRM. Based on topological techniques, we generate 3D maps of local topological features from 3D PRMfSAD classification maps. We found that the surface area of fSAD (SfSAD) was the most robust and significant independent indicator of clinically meaningful measures of COPD. We also confirmed by micro-CT of human lung specimens that structural differences are associated with unique SfSAD patterns, and demonstrated longitudinal feature alterations occurred with worsening pulmonary function independent of an increase in disease extent. These findings suggest that our technique captures additional COPD characteristics, which may provide important opportunities for improved diagnosis of COPD patients.
Conflict of interest statement
E.P. has received an unrestricted educational grant for research from Astra Zeneca and Chiesi; fees for consultancies by E.P. were given to the University of Groningen by A.Z., Boehringer Ingelheim, Chiesi, G.S.K., Nycomed and TEVA. N.H.T.t.H. received grants from GlaxoSmithKline, Boehringer Ingelheim, Nycomed and Chiesi. C.J.G., B.D.R. and B.A.H. have a financial interest in the underlying patented University of Michigan technology licensed to Imbio, L.L.C., a company in which B.D.R. has a financial interest. S.G., P.A.d.J., F.A.A.M.H., L.K., T.D.J., and M.v.d.B. have no competing interests.
Figures
References
-
- Pike, D. et al. Regional Heterogeneity of Chronic Obstructive Pulmonary Disease Phenotypes: Pulmonary He Magnetic Resonance Imaging and Computed Tomography. COPD 1–9 (2016). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
