

Ultrasound and EMG-NCV study (electromyography and nerve conduction velocity) correlation in diagnosis of nerve pathologies
- PMID: 28593000
- PMCID: PMC5440331
- DOI: 10.1007/s40477-016-0232-3
Ultrasound and EMG-NCV study (electromyography and nerve conduction velocity) correlation in diagnosis of nerve pathologies
Abstract
Purpose: Nerve disorders are commonly encountered in clinical practice. Ultrasonography (USG) is a useful modality in the evaluation of most of the peripheral and superficial pathologies amenable to penetration by ultrasound. The primary objective is to study the USG findings of various peripheral nerve pathologies and to correlate them with electrophysiological (EMG-NCV) findings.
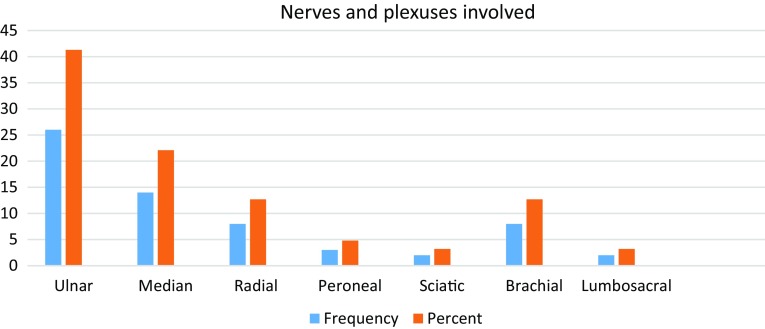
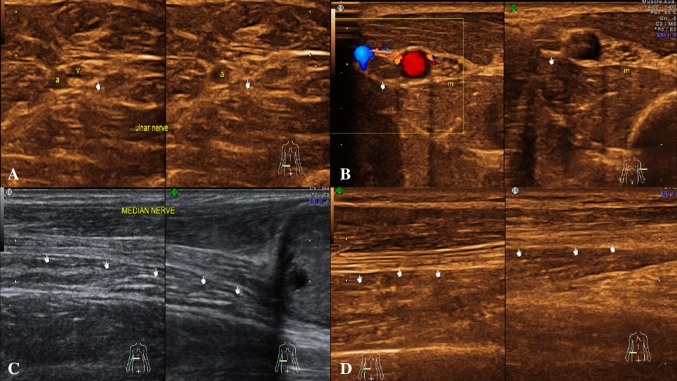
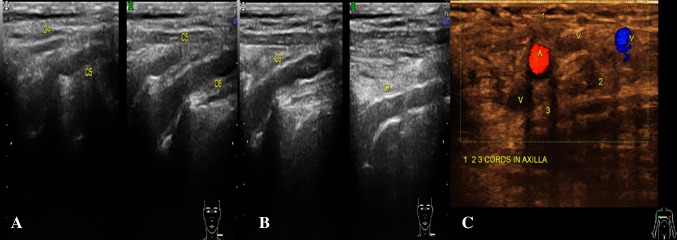
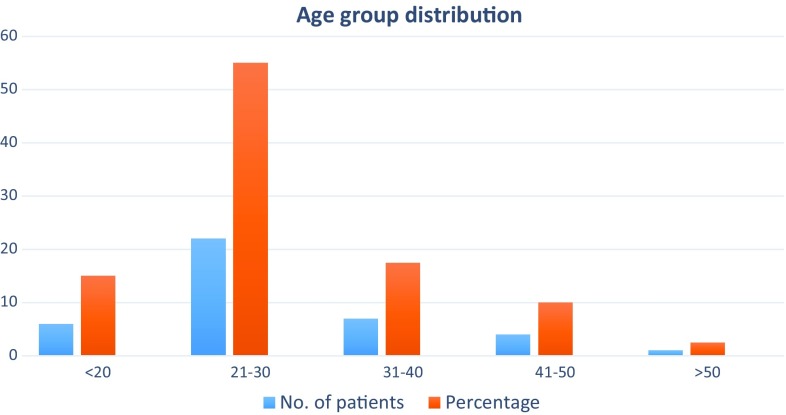
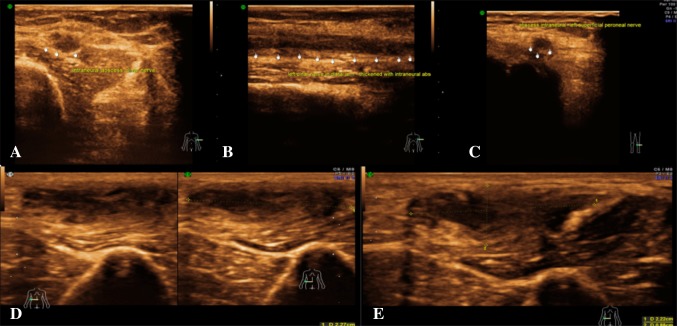
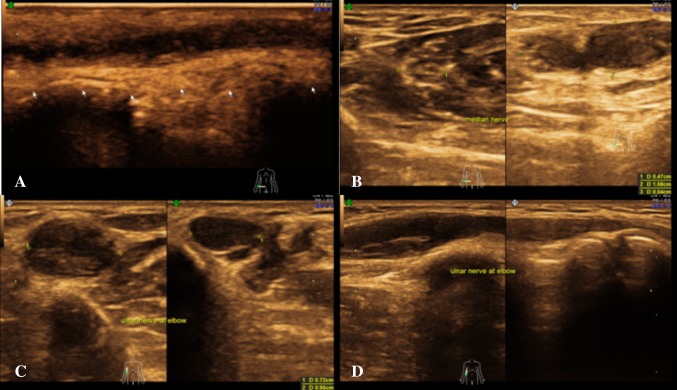
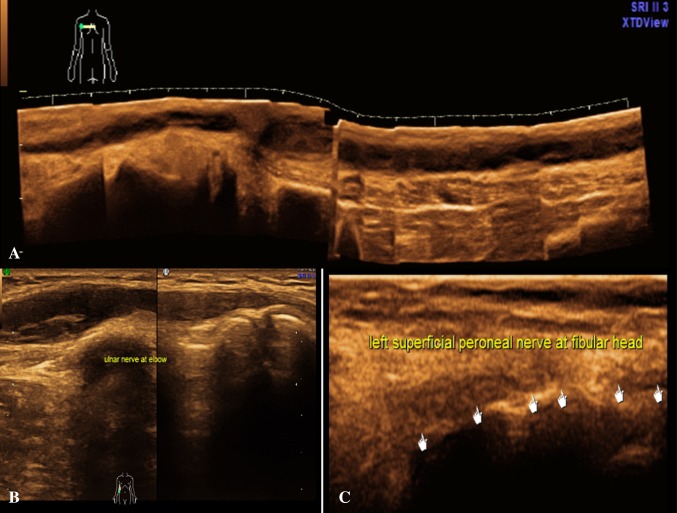
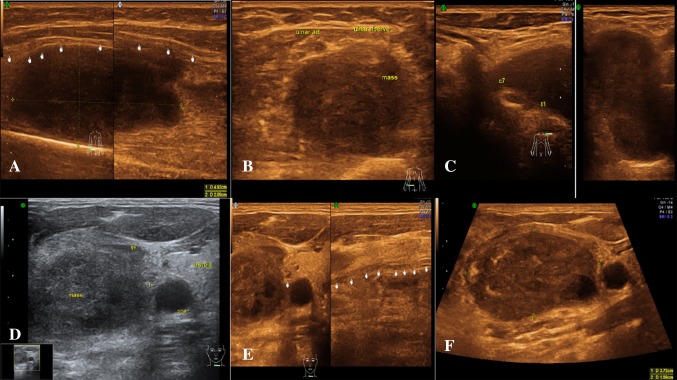
Method: 42 patients referred with suspicion of peripheral nervous system affection were evaluated with USG along with EMG-NCV. After reviewing detailed anatomy of the region, the affected nerve was visualized along the major neurovascular bundle or at a known anatomical landmark with a high-frequency (9-20 MHz) linear/hockey stick transducer.
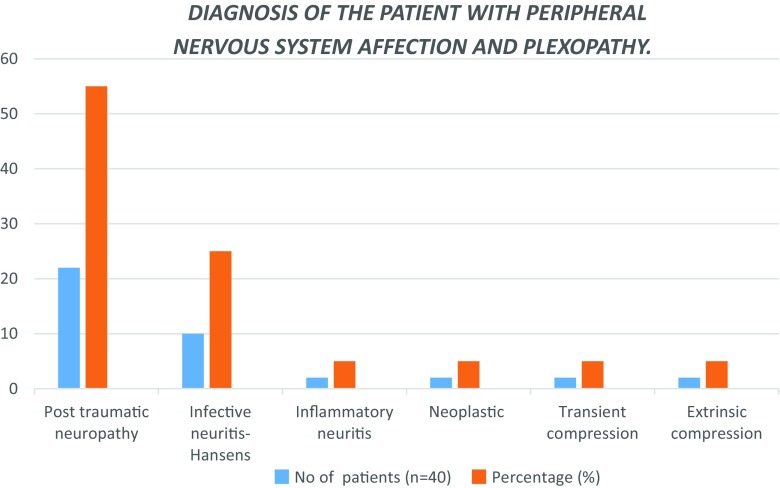
Results: The USG parameters, namely loss of fibrillary pattern, hypoechogenicity and nerve thickening, showed significant p value (p < 0.05) on the tests of significance, suggesting these parameters are significant predictors of nerve affection/pathology on USG. Each ultrasound parameter was correlated individually with SNAP and CMAP. The results revealed positive correlation of echogenicity (r = 0.210, p = 0.05), fibrillary pattern (r = 0.209, p = 0.05) and thickening (r = 0.387, p < 0.05) with sensory nerve action potential (SNAP) and compound muscle action potential (CMAP).
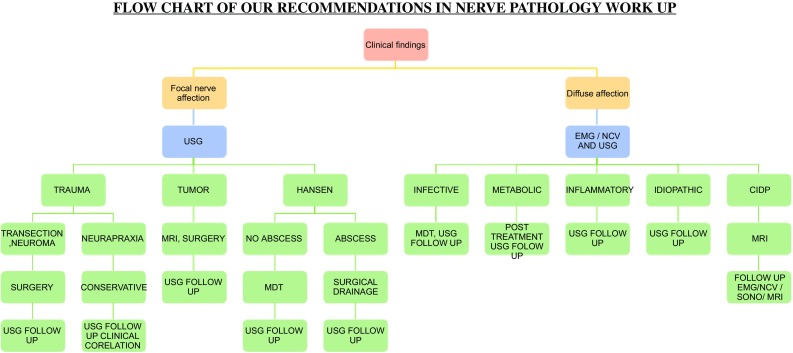
Conclusion: USG can be used as corroborative investigation to strengthen the findings of EMG-NCV. This combination represents a powerful tool in enabling appropriate planning for treatment, preventing unnecessary intervention and thus improving overall outcomes in patients with peripheral neuropathy.
Obiettivo: le malattie neurologiche periferiche sono comuni nella pratica clinica. L’ ecografia (US) è una modalità utile nella valutazione della maggior parte delle patologie periferiche e superficiali. L’ obiettivo primario del lavoro è studiare i reperti delle varie patologie del nervo periferico e correlarli con quelli elettrofisiologici (EMG–NCV).
Metodo: 42 Pazienti con sospette patologie del sistema nervoso periferico sono stati valutati con US ed EMG–NCV. Dopo un dettagliato studio anatomico della regione, il nervo affetto è stato visualizzato lungo tutto il fascio neurovascolare o in prossimità di un repere anatomico noto, con una sonda lineare/hockey stick ad alta frequenza (9-20 MHz).
Risultati: alcuni parametri ecografici quali la perdita del pattern fibrillare, l’ ipoecogenicità e l’ ispessimento del nervo hanno mostrato un p value significativo (p < 0.05), suggerendo che essi sono indicatrori ecografici affidabili della patologia dei nervi. Ogni parametro ecografico è stato correlato singolarmente con il SNAP ed il CMAP. I risultati hanno rivelato una correlazione positiva tra ecogenicità (r = 0.210; p = 0.05), pattern fibrillare (r = 0.209; p = 0.05), ispessimento (r = 0.387; p < 0.05) ed il potenziale d’ azione del nervo sensitivo (SNAP) ed il potenziale d’ azione della componente muscolare.
Conclusioni: L’ ecografia può essere utilizzata come strumento diagnostico aggiuntivo per aumentare l’accuratezza dei reperti EMG–NCV. Questa combinazione rappresenta un valido strumento al fine di programmare il trattamento, prevenire interventi non necessari e conseguentemente migliorare l’ outcome dei Pazienti con neuropatia periferica.
Keywords: CMAP; EMG–NCV; Nerve; SNAP; Trauma; Ultrasound.
Conflict of interest statement
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Figures
Similar articles
-
Preoperative evaluation of peripheral nerve injuries: What is the place for ultrasound?J Neurosurg. 2016 Sep;125(3):603-14. doi: 10.3171/2015.6.JNS151001. Epub 2016 Jan 22. J Neurosurg. 2016. PMID: 26799303
-
[Electrophysiological study of 16 patients with severe N-hexane neuropathy].Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi. 2005 Oct;23(5):351-4. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi. 2005. PMID: 16266512 Chinese.
-
Nerve Conduction Studies and Electromyography.2025 Feb 10. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Feb 10. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 39937950 Free Books & Documents.
-
A non-neurologist's guide to understanding the EMG/NCV report.Clin Podiatr Med Surg. 1999 Jan;16(1):19-28, v. Clin Podiatr Med Surg. 1999. PMID: 9929769 Review.
-
[Neurophysiological evaluation of children with peripheral neuropathy].Rev Neurol. 2002 Aug 1-15;35(3):254-68. Rev Neurol. 2002. PMID: 12235588 Review. Spanish.
Cited by
-
Dorsal ulnar cutaneous nerve conduction study based on nerve ultrasound.Sci Rep. 2024 Sep 3;14(1):20422. doi: 10.1038/s41598-024-71661-3. Sci Rep. 2024. PMID: 39227401 Free PMC article.
-
Considerations about the multidimensional evaluation of a stab wound tibial neuropathy: a case report.J Ultrason. 2023 May 11;23(93):e97-e100. doi: 10.15557/jou.2023.0017. eCollection 2023 Jun. J Ultrason. 2023. PMID: 37520750 Free PMC article.
-
Median neuropathy after multiple punctures of the forearm for catheterization: A case report.World J Clin Cases. 2023 Sep 6;11(25):5941-5946. doi: 10.12998/wjcc.v11.i25.5941. World J Clin Cases. 2023. PMID: 37727486 Free PMC article.
-
Peripheral nerve decompression for pain relief in the setting of previous obstetrical brachial plexus injury: a retrospective case series.Childs Nerv Syst. 2024 Jun;40(6):1813-1819. doi: 10.1007/s00381-024-06348-1. Epub 2024 Mar 8. Childs Nerv Syst. 2024. PMID: 38456921
-
Thoracic outlet syndrome: a rare case with bilateral cervical ribs and bilateral anterior scalene hypertrophy.J Ultrasound. 2021 Sep;24(3):331-336. doi: 10.1007/s40477-019-00418-w. Epub 2019 Dec 13. J Ultrasound. 2021. PMID: 31834601 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
