

Ultrasound detection of aortoenteric fistula in a patient with sepsis
- PMID: 28593006
- PMCID: PMC5440338
- DOI: 10.1007/s40477-017-0249-2
Ultrasound detection of aortoenteric fistula in a patient with sepsis
Abstract
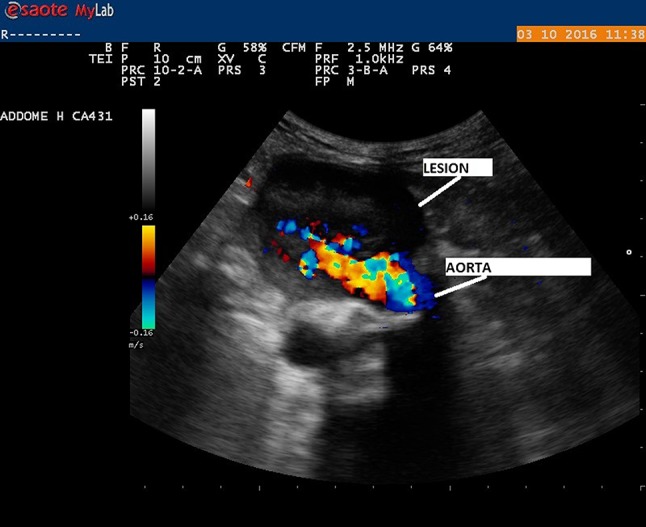
We report a case of an 81-year-old man, hospitalized for sepsis unresponsive to targeted antibiotic therapy, who underwent abdominal aortic aneurysmectomy with stent placement before 12 years. Point-of-care ultrasound examination showed the presence of a voluminous and inhomogeneous lesion adjacent to the anterior wall of aortic bifurcation with pulsatile flow from the aorta into the lesion, highlighted by Color-Doppler, and peripheral (closely with intestinal loops) floating hyperechoic spots marked by posterior comet tail artifact, suggestive for the presence of air bubbles. The presence of an aortoenteric fistula not excluding in differential diagnosis and the possibility of an abscess of aneurysmatic sac with colonization of gas-producing bacteria were suspected; an abdominal contrast-enhanced computed tomography was requested and it confirmed the suspicion of an aortoenteric fistula. The patient underwent emergency surgical intervention with good technical success (evidence of aorto-appendicular fistula), but he died the day after of cardiac arrest.
Descriviamo il caso di un uomo di 81 anni, ricoverato per sepsi non responsiva ad antibioticoterapia mirata, sottoposto 12 anni prima ad aneurismectomia dell'aorta addominale con innesto protesico. L'esame ecografico eseguito al letto mostrava la presenza di una voluminosa formazione disomogenea a livello della parete anteriore della biforcazione aortica, con evidenza, al Color-Doppler, di flusso pulsatile dall'aorta all'interno della lesione, e presenza di spot iperecogeni mobili con artefatto a coda di cometa nella parte più periferica (a stretto contato con le anse intestinali), come per presenza di componente gassosa. Si formulava quindi il sospetto di una fistola aortoenterica, non potendosi escludere, in diagnosi differenziale, una raccolta ascessuale della sacca aneurismatica con colonizzazione di batteri produttori di gas. Veniva richiesta una TC addome urgente con mezzo di contrasto che confermava il sospetto di fistola aorto-enterica; il paziente, veniva sottoposto in urgenza ad intervento chirurgico tecnicamente efficace (riscontro di fistola aorto-appendicolare), ma decedeva nella fase post-operatoria per arresto cardiaco conseguente a infarto miocardico acuto.
Keywords: Abdominal aortic aneurysm; Acute anemia; Aortoenteric fistula; Point of care ultrasound; Sepsis.
Conflict of interest statement
Conflict of interest
The authors Tiziano Perrone MD, Chiara Pagani MD and Elisa Eleonora Mossolani MD, declare that there is no conflict of interest.
Ethical standards
Authors declare that procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration.
Informed consent
The Authors declare that all patients of IRCCS San Matteo of Pavia give at admission written informed consent to analyze in the future their data for research purposes, approved from our Bioethical Committee.
Figures


References
-
- Rosenberg H, Al-Rajhi K (2012) ED ultrasound diagnosis of a type B aortic dissection using the suprasternal view. Am J Emerg Med 30:2084.e1-5- - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
