

Phantosmia and Dysgeusia following Endoscopic Transcribriform Approaches to Olfactory Groove Meningiomas
- PMID: 28593111
- PMCID: PMC5461164
- DOI: 10.1055/s-0036-1597925
Phantosmia and Dysgeusia following Endoscopic Transcribriform Approaches to Olfactory Groove Meningiomas
Abstract
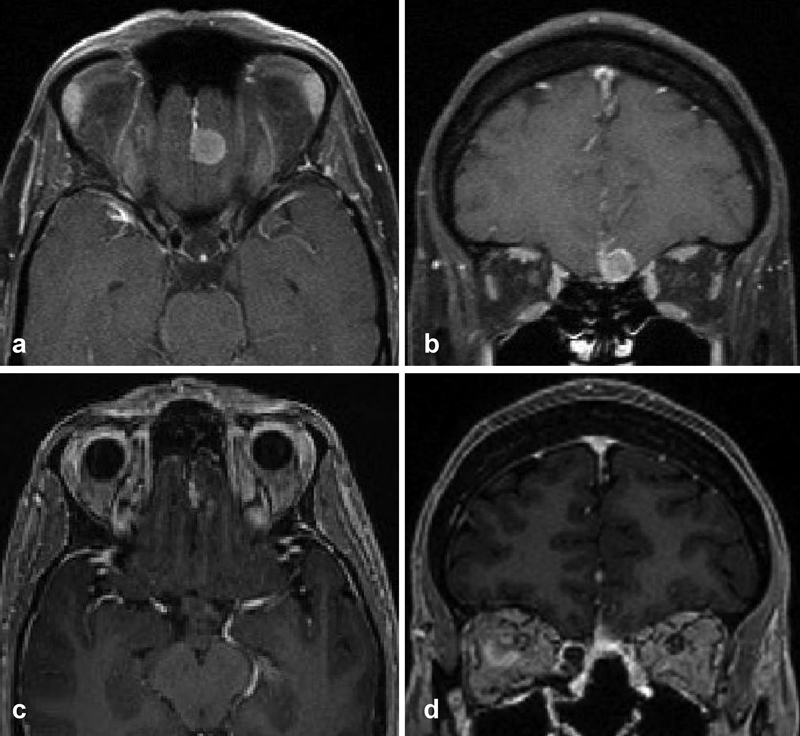
The endoscopic, endonasal transcribriform approach (EETA) is an important technique used to directly access the anterior skull base and is increasingly being used in the management of olfactory groove meningiomas (OGMs). As this approach requires removal of the cribriform plate and olfactory epithelium en route to the tumor, patients are anosmic postoperatively. Here, we report the development of phantosmia and dysgeusia in two patients who underwent EETAs for OGMs, which has not yet been reported in the literature. We hypothesize that phantosmia and dysgeusia may result from aberrant neuronal signals or misinterpretation centrally from the remaining distal portions of the olfactory and taste pathways. Since EETAs are newer than traditional open craniotomy-based techniques, reporting these outcomes will be important to appropriately counsel patients preoperatively.
Keywords: anterior skull base; dysgeusia; olfactory groove meningioma; phantosmia; transcribriform.
Figures

Similar articles
-
How I Do It: Endonasal transethmoidal, transcribriform approach for resection of giant olfactory groove meningioma.Acta Neurochir (Wien). 2022 Nov;164(11):2981-2985. doi: 10.1007/s00701-022-05308-5. Epub 2022 Jul 7. Acta Neurochir (Wien). 2022. PMID: 35794428
-
Endoscopic Endonasal Approach for Olfactory Groove Meningiomas: Operative Technique and Nuances.Neurosurg Clin N Am. 2015 Jul;26(3):377-88. doi: 10.1016/j.nec.2015.03.009. Neurosurg Clin N Am. 2015. PMID: 26141357 Review.
-
Unilateral endonasal transcribriform approach with septal transposition for olfactory groove meningioma: can olfaction be preserved?Acta Neurochir (Wien). 2016 Oct;158(10):1965-72. doi: 10.1007/s00701-016-2922-1. Epub 2016 Aug 26. Acta Neurochir (Wien). 2016. PMID: 27562683
-
Expanded endoscopic endonasal transcribriform approach for resection of anterior skull base olfactory schwannoma.Neurosurg Focus. 2012 Jan;32 Suppl 1:E3. doi: 10.3171/2012.V3.FOCUS11300. Neurosurg Focus. 2012. PMID: 26018973
-
Limitations of the endoscopic endonasal transcribriform approach.J Neurosurg Sci. 2018 Jun;62(3):287-296. doi: 10.23736/S0390-5616.18.04348-5. Epub 2018 Feb 13. J Neurosurg Sci. 2018. PMID: 29444558 Review.
Cited by
-
Smell Preservation following Unilateral Endoscopic Transnasal Approach to Resection of Olfactory Groove Meningioma: A Multi-institutional Experience.J Neurol Surg B Skull Base. 2020 Jun;81(3):263-267. doi: 10.1055/s-0039-1688794. Epub 2019 May 28. J Neurol Surg B Skull Base. 2020. PMID: 32500000 Free PMC article.
-
Olfaction preservation in olfactory groove meningiomas: a systematic review.Neurosurg Rev. 2023 Jul 27;46(1):186. doi: 10.1007/s10143-023-02096-z. Neurosurg Rev. 2023. PMID: 37500988 Free PMC article.
-
Olfactory Outcomes after Resection of Tuberculum Sella and Planum Sphenoidale Meningiomas via a Transcranial Approach.J Neurol Surg B Skull Base. 2021 Jan 21;83(3):296-304. doi: 10.1055/s-0040-1722671. eCollection 2022 Jun. J Neurol Surg B Skull Base. 2021. PMID: 35769800 Free PMC article.
References
-
- Bakay L. Olfactory meningiomas. The missed diagnosis. JAMA. 1984;251(01):53–55. - PubMed
-
- Hentschel S J, DeMonte F. Olfactory groove meningiomas. Neurosurg Focus. 2003;14(06):e4. - PubMed
-
- Zygourakis C C, Sughrue M E, Benet A, Parsa A T, Berger M S, McDermott M W. Management of planum/olfactory meningiomas: predicting symptoms and postoperative complications. World Neurosurg. 2014;82(06):1216–1223. - PubMed
-
- Nakamura M, Struck M, Roser F, Vorkapic P, Samii M.Olfactory groove meningiomas: clinical outcome and recurrence rates after tumor removal through the frontolateral and bifrontal approach Neurosurgery 20086206, (suppl 3)1224–1232. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
