

Simultaneous Antidepressant and Benzodiazepine New Use and Subsequent Long-term Benzodiazepine Use in Adults With Depression, United States, 2001-2014
- PMID: 28593281
- PMCID: PMC5710248
- DOI: 10.1001/jamapsychiatry.2017.1273
Simultaneous Antidepressant and Benzodiazepine New Use and Subsequent Long-term Benzodiazepine Use in Adults With Depression, United States, 2001-2014
Abstract
Importance: Benzodiazepines have been prescribed for short periods to patients with depression who are beginning antidepressant therapy to improve depressive symptoms more quickly, mitigate concomitant anxiety, and improve antidepressant treatment continuation. However, benzodiazepine therapy is associated with risks, including dependency, which may take only a few weeks to develop.
Objectives: To examine trends in simultaneous benzodiazepine and antidepressant new use among adults with depression initiating an antidepressant, assess antidepressant treatment length by simultaneous new use status, estimate subsequent long-term benzodiazepine use in those with simultaneous antidepressant and benzodiazepine new use, and identify determinants of simultaneous new use and long-term benzodiazepine use.
Design, setting, and participants: This cohort study using a US commercial claims database included commercially insured adults (aged 18-64 years) from January 1, 2001, through December 31, 2014, with a recent depression diagnosis who began antidepressant therapy but had not used antidepressants or benzodiazepines in the prior year.
Exposures: Simultaneous new use, defined as a new benzodiazepine prescription dispensed on the same day as a new antidepressant prescription.
Main outcomes and measures: The proportion of antidepressant initiators with simultaneous new use and continuing antidepressant treatment for 6 months and the proportion of simultaneous new users receiving long-term (6-months) benzodiazepine therapy.
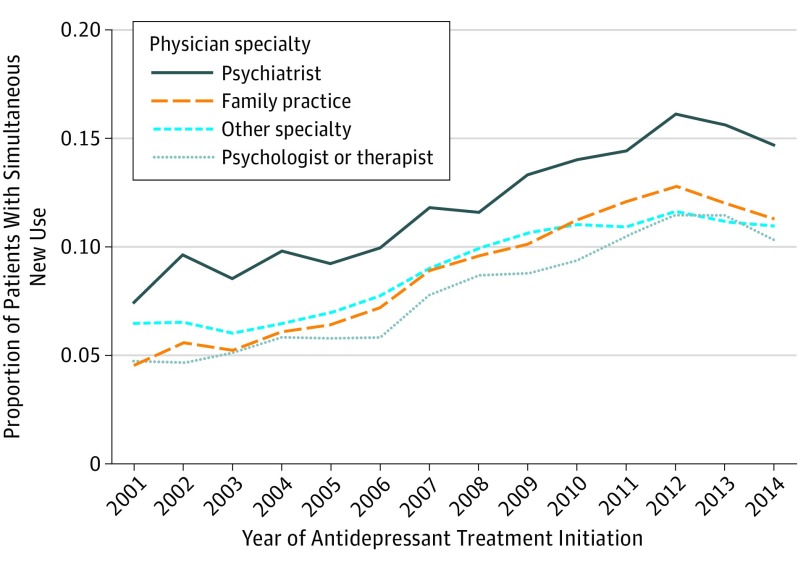
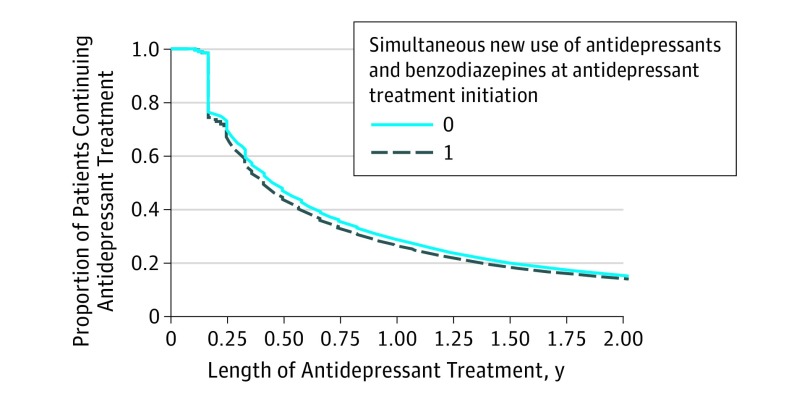
Results: Of the 765 130 adults (median age, 39 years; interquartile range, 29-49 years; 507 451 women [66.3%]) who initiated antidepressant treatment, 81 020 (10.6%) also initiated benzodiazepine treatment. The mean annual increase in the proportion simultaneously starting use of both agents from 2001 to 2014 was 0.49% (95% CI, 0.47%-0.51%), increasing from 6.1% (95% CI, 5.5%-6.6%) in 2001 to 12.5% (95% CI, 12.3%-12.7%) in 2012 and stabilizing through 2014 (11.3%; 95% CI, 11.1%-11.5%). Similar findings were apparent by age group and physician type. Antidepressant treatment length was similar in simultaneous new users and non-simultaneous new users. Among simultaneous new users, 12.3% (95% CI, 12.0%-12.5%) exhibited long-term benzodiazepine use (64.0% discontinued taking benzodiazepines after the initial fill). Determinants of long-term benzodiazepine use after simultaneous new use were longer initial benzodiazepine days' supply, first prescription for a long-acting benzodiazepine, and recent prescription opioid fills.
Conclusions and relevance: One-tenth of antidepressant initiators with depression simultaneously initiated benzodiazepine therapy. No meaningful difference in antidepressant treatment at 6 months was observed by simultaneous new use status. Because of the risks associated with benzodiazepines, simultaneous new use at antidepressant initiation and the benzodiazepine regimen itself require careful consideration.
Conflict of interest statement
Figures
Similar articles
-
Who diagnosed and prescribed what? Using provider details to inform observational research.Pharmacoepidemiol Drug Saf. 2018 Dec;27(12):1422-1426. doi: 10.1002/pds.4685. Epub 2018 Oct 31. Pharmacoepidemiol Drug Saf. 2018. PMID: 30379369 Free PMC article.
-
Benzodiazepine use in the United States.JAMA Psychiatry. 2015 Feb;72(2):136-42. doi: 10.1001/jamapsychiatry.2014.1763. JAMA Psychiatry. 2015. PMID: 25517224
-
Rates of Physician Coprescribing of Opioids and Benzodiazepines After the Release of the Centers for Disease Control and Prevention Guidelines in 2016.JAMA Netw Open. 2019 Aug 2;2(8):e198325. doi: 10.1001/jamanetworkopen.2019.8325. JAMA Netw Open. 2019. PMID: 31373650 Free PMC article.
-
Understanding the effects of chronic benzodiazepine use in depression: a focus on neuropharmacology.Int Clin Psychopharmacol. 2020 Sep;35(5):243-253. doi: 10.1097/YIC.0000000000000316. Int Clin Psychopharmacol. 2020. PMID: 32459725 Review.
-
Benzodiazepine Prescribing in People with Chronic Obstructive Pulmonary Disease: Clinical Considerations.Drugs Aging. 2020 Apr;37(4):263-270. doi: 10.1007/s40266-020-00756-z. Drugs Aging. 2020. PMID: 32107742 Review.
Cited by
-
Simultaneous Benzodiazepine and SSRI Initiation in Young People With Anxiety Disorders.J Clin Psychiatry. 2021 Oct 19;82(6):20m13863. doi: 10.4088/JCP.20m13863. J Clin Psychiatry. 2021. PMID: 34670029 Free PMC article.
-
Drug overdose risk with benzodiazepine treatment in young adults: Comparative analysis in privately and publicly insured individuals.Addiction. 2024 Feb;119(2):356-368. doi: 10.1111/add.16359. Epub 2023 Oct 10. Addiction. 2024. PMID: 37816665 Free PMC article.
-
Influence of SSRI and SNRI co-prescription on benzodiazepine prescription trajectories.Drug Alcohol Depend Rep. 2025 Mar 18;15:100325. doi: 10.1016/j.dadr.2025.100325. eCollection 2025 Jun. Drug Alcohol Depend Rep. 2025. PMID: 40226211 Free PMC article.
-
Safety, effectiveness and tolerability of sublingual ketamine in depression and anxiety: A retrospective study of off-label, at-home use.Front Psychiatry. 2022 Sep 28;13:992624. doi: 10.3389/fpsyt.2022.992624. eCollection 2022. Front Psychiatry. 2022. PMID: 36245861 Free PMC article.
-
Incident Benzodiazepine and Z-Drug Use and Subsequent Risk of Serious Infections.CNS Drugs. 2024 Oct;38(10):827-838. doi: 10.1007/s40263-024-01108-w. Epub 2024 Aug 1. CNS Drugs. 2024. PMID: 39090338 Free PMC article.
References
-
- American Psychiatric Association Practice Guideline for the Treatment of Patients With Major Depressive Disorder. 3rd ed Arlington, VA: American Psychiatric Association; 2010.
-
- Furukawa TA, Streiner DL, Young LT, Kinoshita Y. Antidepressant plus benzodiazepine for major depression. Cochrane Database Syst Rev. 2001;2(2):CD001026. - PubMed
-
- Smith WT, Londborg PD, Glaudin V, Painter JR; Summit Research Network . Is extended clonazepam cotherapy of fluoxetine effective for outpatients with major depression? J Affect Disord. 2002;70(3):251-259. - PubMed
-
- Youssef NA, Rich CL. Does acute treatment with sedatives/hypnotics for anxiety in depressed patients affect suicide risk? a literature review. Ann Clin Psychiatry. 2008;20(3):157-169. - PubMed
-
- Baldwin DS, Aitchison K, Bateson A, et al. . Benzodiazepines: risks and benefits: a reconsideration. J Psychopharmacol. 2013;27(11):967-971. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
