

Intraoperative Infusion of Dexmedetomidine for Prevention of Postoperative Delirium and Cognitive Dysfunction in Elderly Patients Undergoing Major Elective Noncardiac Surgery: A Randomized Clinical Trial
- PMID: 28593326
- PMCID: PMC5831461
- DOI: 10.1001/jamasurg.2017.1505
Intraoperative Infusion of Dexmedetomidine for Prevention of Postoperative Delirium and Cognitive Dysfunction in Elderly Patients Undergoing Major Elective Noncardiac Surgery: A Randomized Clinical Trial
Abstract
Importance: Postoperative delirium occurs in 10% to 60% of elderly patients having major surgery and is associated with longer hospital stays, increased hospital costs, and 1-year mortality. Emerging literature suggests that dexmedetomidine sedation in critical care units is associated with reduced incidence of delirium. However, intraoperative use of dexmedetomidine for prevention of delirium has not been well studied.
Objective: To evaluate whether an intraoperative infusion of dexmedetomidine reduces postoperative delirium.
Design, setting, and participants: This study was a multicenter, double-blind, randomized, placebo-controlled trial that randomly assigned patients to dexmedetomidine or saline placebo infused during surgery and for 2 hours in the recovery room. Patients were assessed daily for postoperative delirium (primary outcome) and secondarily for postoperative cognitive decline. Participants were elderly (>68 years) patients undergoing major elective noncardiac surgery. The study dates were February 2008 to May 2014.
Interventions: Dexmedetomidine infusion (0.5 µg/kg/h) during surgery and up to 2 hours in the recovery room.
Main outcomes and measures: The primary hypothesis tested was that intraoperative dexmedetomidine administration would reduce postoperative delirium. Secondarily, the study examined the correlation between dexmedetomidine use and postoperative cognitive change.
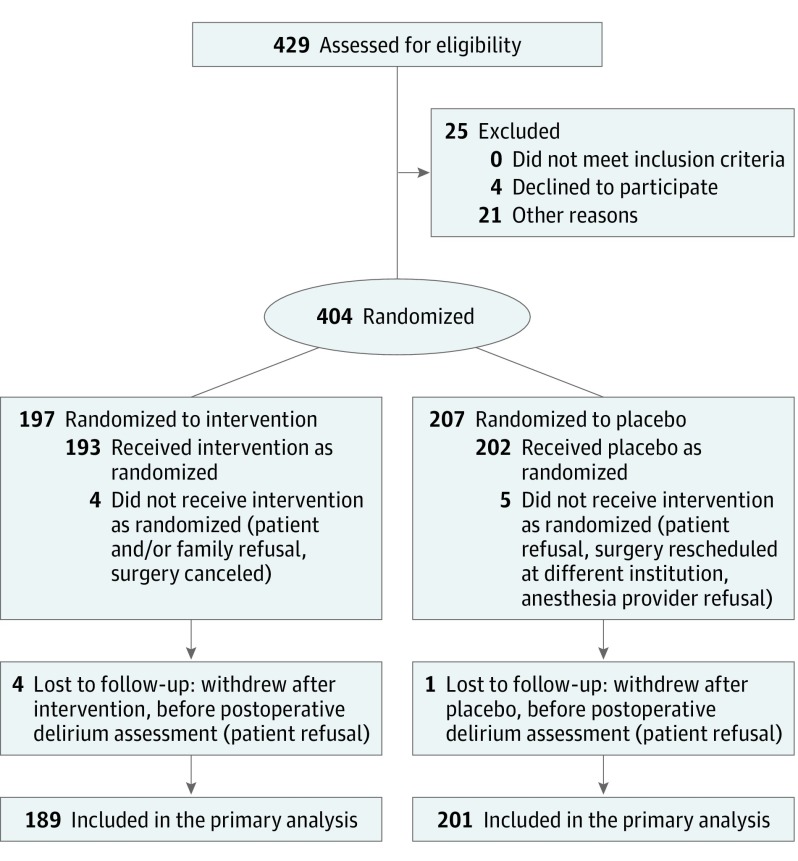
Results: In total, 404 patients were randomized; 390 completed in-hospital delirium assessments (median [interquartile range] age, 74.0 [71.0-78.0] years; 51.3% [200 of 390] female). There was no difference in postoperative delirium between the dexmedetomidine and placebo groups (12.2% [23 of 189] vs 11.4% [23 of 201], P = .94). After adjustment for age and educational level, there was no difference in the postoperative cognitive performance between treatment groups at 3 months and 6 months. Adverse events were comparably distributed in the treatment groups.
Conclusions and relevance: Intraoperative dexmedetomidine does not prevent postoperative delirium. The reduction in delirium previously demonstrated in numerous surgical intensive care unit studies was not observed, which underscores the importance of timing when administering the drug to prevent delirium.
Trial registration: clinicaltrials.gov Identifier NCT00561678.
Conflict of interest statement
Figures
Comment in
-
Confusion Regarding Surgical Delirium-Is Dexmedetomidine the Answer?JAMA Surg. 2017 Aug 16;152(8):e171511. doi: 10.1001/jamasurg.2017.1511. Epub 2017 Aug 16. JAMA Surg. 2017. PMID: 28593269 No abstract available.
References
-
- Müller A, Lachmann G, Wolf A, Mörgeli R, Weiss B, Spies C. Peri- and postoperative cognitive and consecutive functional problems of elderly patients. Curr Opin Crit Care. 2016;22(4):406-411. - PubMed
-
- Inouye SK. Delirium in older persons. N Engl J Med. 2006;354(11):1157-1165. - PubMed
-
- American Geriatrics Society Expert Panel on Postoperative Delirium in Older Adults Postoperative delirium in older adults: best practice statement from the American Geriatrics Society. J Am Coll Surg. 2015;220(2):136-148.e1. - PubMed
-
- Evered L, Scott DA, Silbert B, Maruff P. Postoperative cognitive dysfunction is independent of type of surgery and anesthetic. Anesth Analg. 2011;112(5):1179-1185. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
