

The Importance of Registries in the Postmarketing Surveillance of Surgical Meshes
- PMID: 28594740
- PMCID: PMC6250300
- DOI: 10.1097/SLA.0000000000002326
The Importance of Registries in the Postmarketing Surveillance of Surgical Meshes
Abstract
Objective: To assess the role of registries in the postmarketing surveillance of surgical meshes.
Background: To date, surgical meshes are classified as group II medical devices. Class II devices do not require premarket clearance by clinical studies. Ethicon initiated a voluntary market withdrawal of Physiomesh for laparoscopic use after an analysis of unpublished data from the 2 large independent hernia registries-Herniamed German Registry and Danish Hernia Database. This paper now presents the relevant data from the Herniamed Registry.
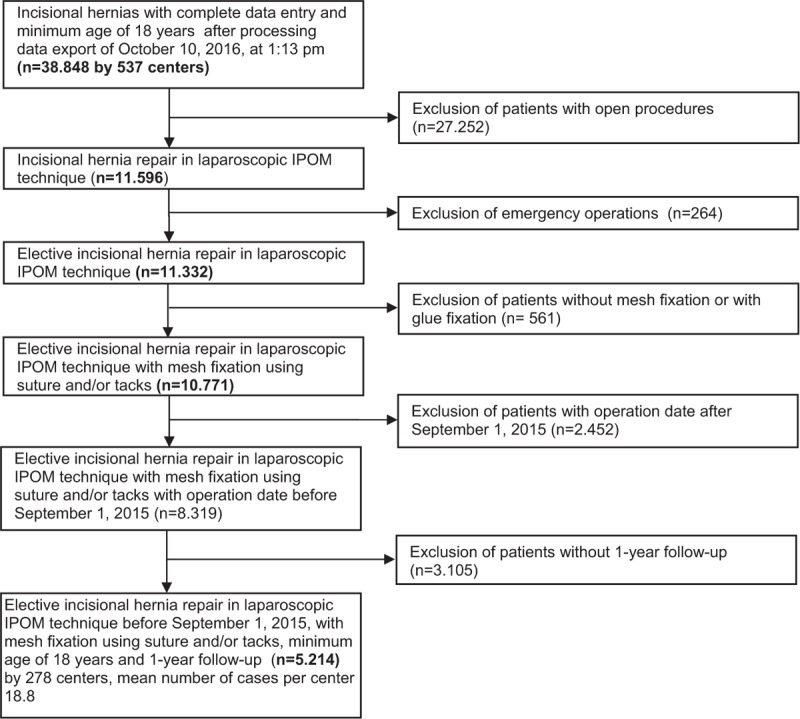
Methods: The present analysis compares the prospective perioperative and 1-year follow-up data collected for all patients with incisional hernia who had undergone elective laparoscopic intraperitoneal onlay mesh repair either with Physiomesh (n = 1380) or with other meshes recommended in the guidelines (n = 3834).
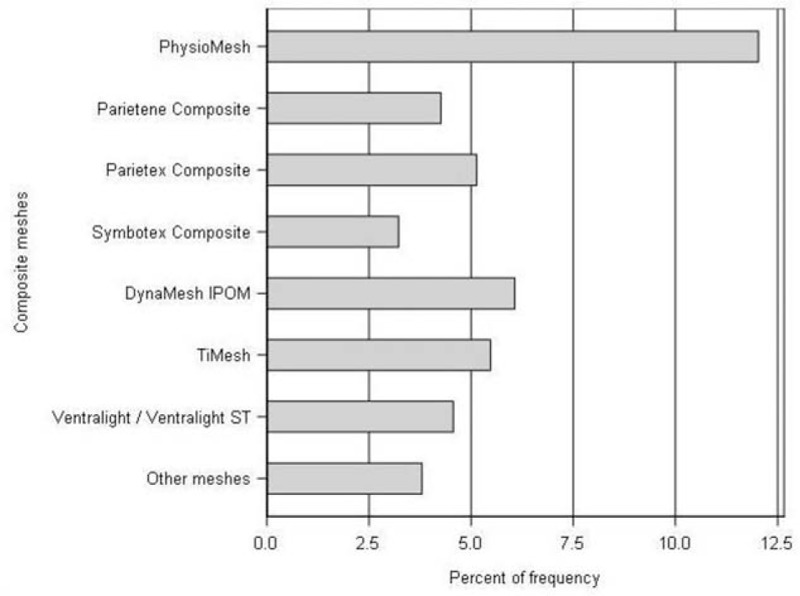
Results: Patients with Physiomesh repair had a markedly higher recurrence rate compared with the other recommended meshes (12.0% vs 5.0%; P < 0.001). In the multivariable analysis, the recurrence rate was highly significantly influenced by the mesh type used (P < 0.001). If Physiomesh was used, that led to a highly significant increase in the recurrence rate on 1-year follow-up (odds ratio 2.570, 95% CI 2.057, 3.210). The mesh type used also had a significant influence on chronic pain rates.
Conclusions: The importance of real-world data for postmarketing surveillance of surgical meshes has been demonstrated in this registry-based study. Randomized controlled trials are needed for premarket approval of new devices. The role of sponsorship of device studies by the manufacturing company must be taken into account.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
Comment in
-
Surveillance of Surgical Meshes in Ventral Hernias and Unpredictability of Their History.Ann Surg. 2018 Apr;267(4):e65. doi: 10.1097/SLA.0000000000002537. Ann Surg. 2018. PMID: 29112002
-
Response to Comment on "the Study by Melkemichel: Long-term Comparison of Recurrence Rates Between Different Lightweight and Heavyweight Meshes in Open Anterior Mesh Inguinal Hernia Repair-A Nationwide Population-based Register Study".Ann Surg. 2019 Dec;270(6):e116-e117. doi: 10.1097/SLA.0000000000003311. Ann Surg. 2019. PMID: 30946075 No abstract available.
-
Comment on "Study of Melkemichel Long-term Comparison of Recurrence Rates Between Different Lightweight and Heavyweight Meshes in Open Anterior Mesh Inguinal Hernia Repair: A Nationwide Population-based Register Study".Ann Surg. 2019 Dec;270(6):e115-e116. doi: 10.1097/SLA.0000000000003312. Ann Surg. 2019. PMID: 31058702 No abstract available.
References
-
- Sauerland S, Walgenbach M, Habermalz B, et al. Laparoscopic versus open surgical techniques for ventral or incisional hernia repair. Cochrane Database Syst Rev 2011; CD007781. - PubMed
-
- Zhang Y, Zhou H, Chai Y, et al. Laparoscopic versus open incisional and ventral hernia repair: a systematic review and meta-analysis. World J Surg 2014; 38:2233–2240. - PubMed
-
- Al Chalabi H, Larkin J, Mehigan B, et al. A systematic review of laparoscopic versus open abdominal incisional hernia repair, with meta-analysis of randomized controlled trials. Int J Surg 2015; 20:65–74. - PubMed
-
- Awaiz A, Rahman F, Hossain MB, et al. Meta-analysis and systematic review of laparoscopic versus open mesh repair for elective incisional hernia. Hernia 2015; 19:449–463. - PubMed
-
- Jensen KK, Jorgensen LN. Comment to: Meta-analysis and systematic review of laparoscopic versus open mesh repair for elective incisional hernia [Awaiz A et al. Hernia 2015; 19: 449–463]. Hernia 2015; 19:1025–1026. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
