

Obstructive Sleep Apnea Dynamically Increases Nocturnal Plasma Free Fatty Acids, Glucose, and Cortisol During Sleep
- PMID: 28595341
- PMCID: PMC5587067
- DOI: 10.1210/jc.2017-00619
Obstructive Sleep Apnea Dynamically Increases Nocturnal Plasma Free Fatty Acids, Glucose, and Cortisol During Sleep
Abstract
Context: Obstructive sleep apnea (OSA) is associated with diabetes and cardiovascular disease. This association may be related to metabolic changes that transpire during sleep in OSA.
Objective: To examine the impact of OSA, elicited by cessation of continuous positive airway pressure (CPAP), on frequently sampled nocturnal metabolic markers including plasma free fatty acids (FFAs), glucose, insulin, triglycerides (TGs), cortisol, and lactate, as well as glucose production, oral glucose tolerance, blood pressure (BP), endothelial function, cholesterol, and high-sensitivity C-reactive protein (hsCRP).
Design and setting: Randomized crossover trial of CPAP vs CPAP withdrawal.
Patients: Thirty-one patients with moderate to severe OSA acclimated to CPAP.
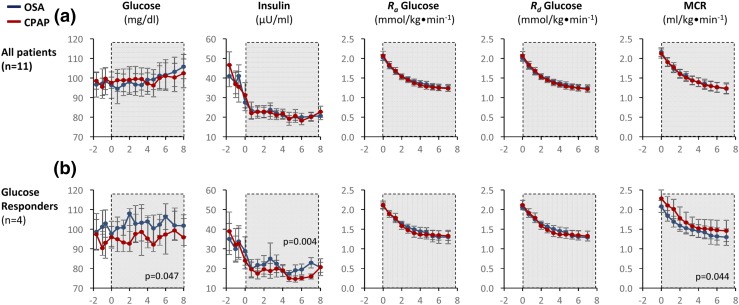
Intervention: Patients underwent attended polysomnography while sleeping with therapeutic CPAP, or after CPAP withdrawal, in random order. Venous blood was sampled at ∼20-minute intervals on both nights. In 11 patients, we assessed glucose kinetics with an infusion of 6,6-[2H2]glucose.
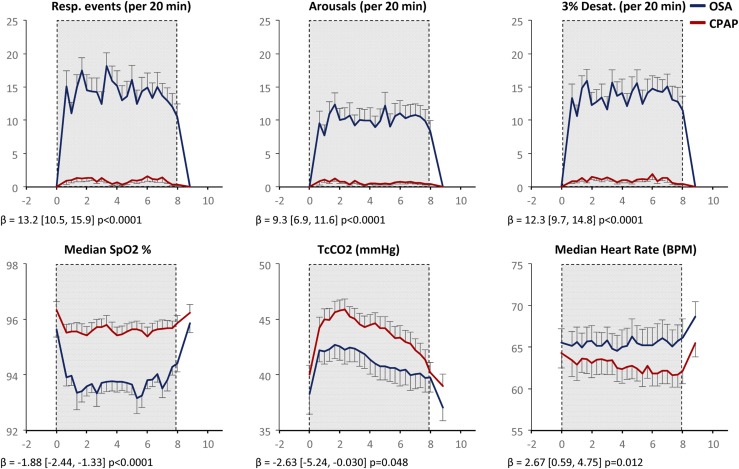
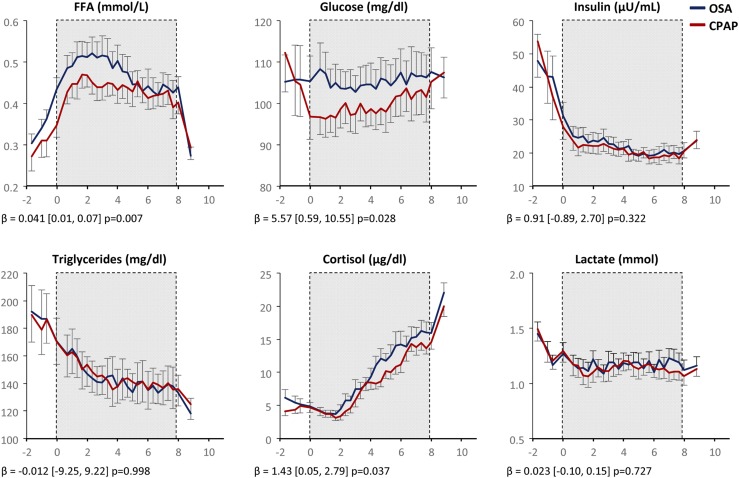
Results: CPAP withdrawal caused recurrence of OSA associated with hypoxemia, sleep disruption, and heart rate (HR) elevation. CPAP withdrawal dynamically increased nocturnal FFA (P = 0.007), glucose (P = 0.028), and cortisol (P = 0.037), in proportion to respiratory event frequency, HR elevation, or sleep fragmentation. Diabetes predisposed to glucose elevation. CPAP withdrawal also increased systolic BP (P = 0.017) and augmentation index (P = 0.008), but did not affect insulin, TGs, glucose production, oral glucose tolerance, cholesterol, or hsCRP.
Conclusion: OSA recurrence during CPAP withdrawal increases FFA and glucose during sleep, associated with sympathetic and adrenocortical activation. Recurring exposure to these metabolic changes may foster diabetes and cardiovascular disease.
Trial registration: ClinicalTrials.gov NCT02824263.
Copyright © 2017 Endocrine Society
Figures
References
-
- Bonsignore MR, Marrone O, Insalaco G, Bonsignore G. The cardiovascular effects of obstructive sleep apnoeas: analysis of pathogenic mechanisms. Eur Respir J. 1994;7(4):786–805. - PubMed
-
- Alzoghaibi MA, Bahammam AS. The effect of one night of continuous positive airway pressure therapy on oxidative stress and antioxidant defense in hypertensive patients with severe obstructive sleep apnea. Sleep Breath. 2012;16:499–504. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
