

Incretin based treatments and mortality in patients with type 2 diabetes: systematic review and meta-analysis
- PMID: 28596247
- PMCID: PMC5463186
- DOI: 10.1136/bmj.j2499
Incretin based treatments and mortality in patients with type 2 diabetes: systematic review and meta-analysis
Abstract
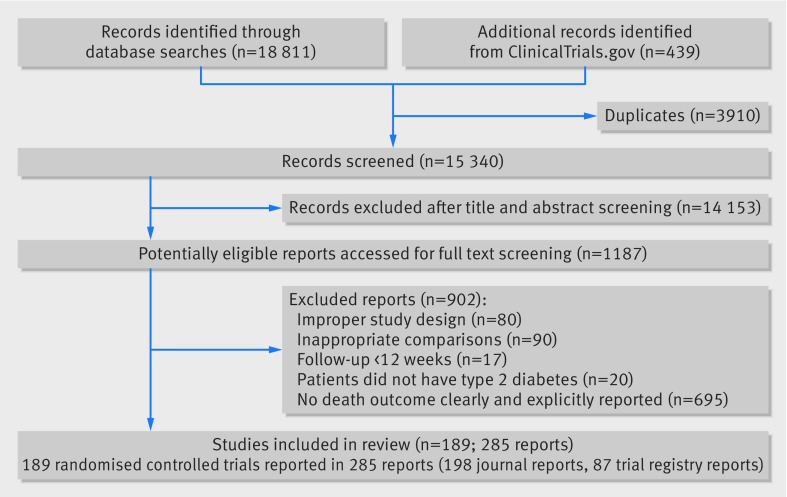
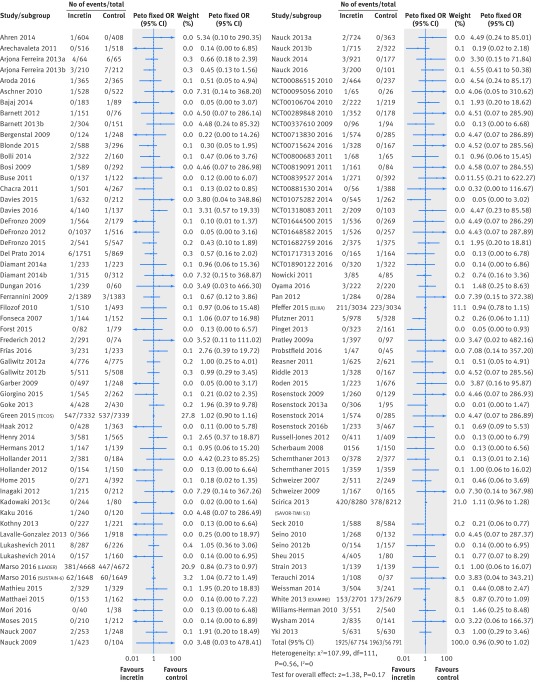
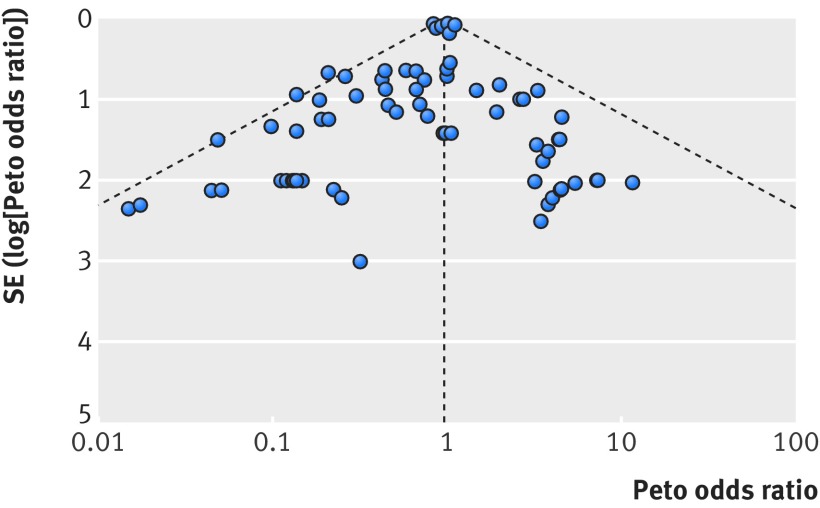
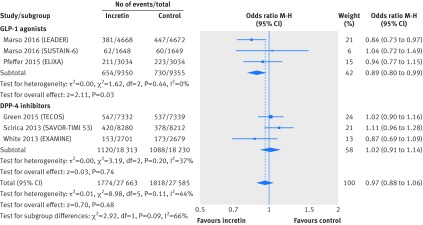
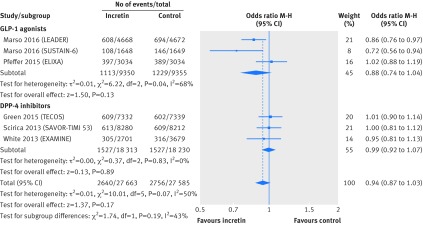
Objective To assess the impact of incretin based treatment on all cause mortality in patients with type 2 diabetes.Design Systematic review and meta-analysis of randomised trials.Data sources Medline, Embase, the Cochrane Central Register of Controlled Trials (CENTRAL), and ClinicalTrials.gov.Eligibility criteria Randomised controlled trials that compared glucagon-like peptide-1 (GLP-1) receptor agonists or dipeptidyl peptidase-4 (DPP-4) inhibitors with placebo or active anti-diabetic drugs in patients with type 2 diabetes.Data collection and analysis Paired reviewers independently screened citations, assessed risk of bias of included studies, and extracted data. Peto's method was used as the primary approach to pool effect estimates from trials, sensitivity analyses were carried out with other statistical approaches, and meta-regression was applied for six prespecified hypotheses to explore heterogeneity. The GRADE approach was used to rate the quality of evidence.Results 189 randomised controlled trials (n=155 145) were included, all of which were at low to moderate risk of bias; 77 reported no events of death and 112 reported 3888 deaths among 151 614 patients. Meta-analysis of 189 trials showed no difference in all cause mortality between incretin drugs versus control (1925/84 136 v 1963/67 478; odds ratio 0.96, 95% confidence interval 0.90 to 1.02, I2=0%; risk difference 3 fewer events (95% confidence interval 7 fewer to 1 more) per 1000 patients over five years; moderate quality evidence). Results suggested the possibility of a mortality benefit with GLP-1 agonists but not DPP-4 inhibitors, but the subgroup hypothesis had low credibility. Sensitivity analyses showed no important differences in the estimates of effects.Conclusions Current evidence does not support the suggestion that incretin based treatment increases all cause mortality in patients with type 2 diabetes. Further studies are warranted to examine if the effect differs between GLP-1 agonists versus DPP-4 inhibitors.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years, and no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Nauck M. Incretin therapies: highlighting common features and differences in the modes of action of glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors. Diabetes Obes Metab 2016;18:203-16. 10.1111/dom.12591 pmid:26489970. - DOI - PMC - PubMed
-
- Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes, 2015: a patient-centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2015;38:140-9. 10.2337/dc14-2441 pmid:25538310. - DOI - PubMed
-
- Tricco AC, Antony J, Khan PA, et al. Safety and effectiveness of dipeptidyl peptidase-4 inhibitors versus intermediate-acting insulin or placebo for patients with type 2 diabetes failing two oral antihyperglycaemic agents: a systematic review and network meta-analysis. BMJ Open 2014;4:e005752 10.1136/bmjopen-2014-005752 pmid:25537781. - DOI - PMC - PubMed
-
- Karagiannis T, Paschos P, Paletas K, Matthews DR, Tsapas A. Dipeptidyl peptidase-4 inhibitors for treatment of type 2 diabetes mellitus in the clinical setting: systematic review and meta-analysis. BMJ 2012;344:e1369 10.1136/bmj.e1369 pmid:22411919. - DOI - PubMed
-
- Aroda VR, Henry RR, Han J, et al. Efficacy of GLP-1 receptor agonists and DPP-4 inhibitors: meta-analysis and systematic review. Clin Ther 2012;34:1247-1258.e22. 10.1016/j.clinthera.2012.04.013 pmid:22608780. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous