

HLA-DRB1*07:01-HLA-DQA1*02:01-HLA-DQB1*02:02 haplotype is associated with a high risk of asparaginase hypersensitivity in acute lymphoblastic leukemia
- PMID: 28596278
- PMCID: PMC5685222
- DOI: 10.3324/haematol.2017.168211
HLA-DRB1*07:01-HLA-DQA1*02:01-HLA-DQB1*02:02 haplotype is associated with a high risk of asparaginase hypersensitivity in acute lymphoblastic leukemia
Abstract
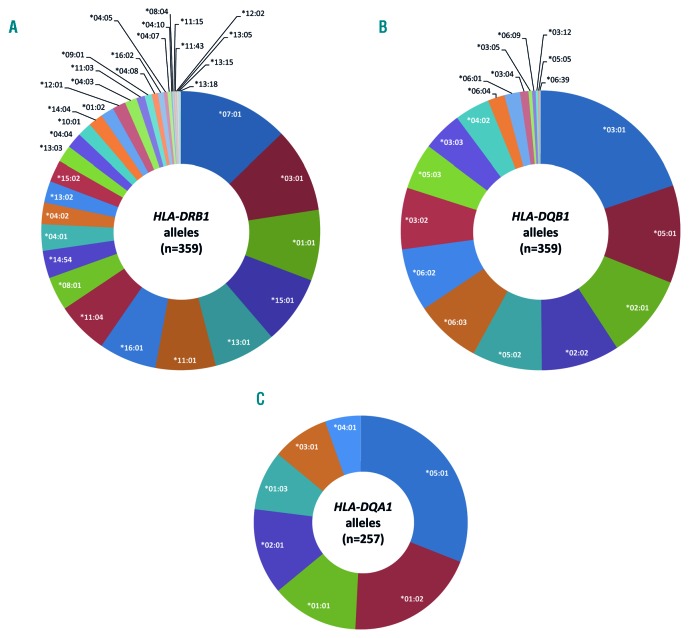
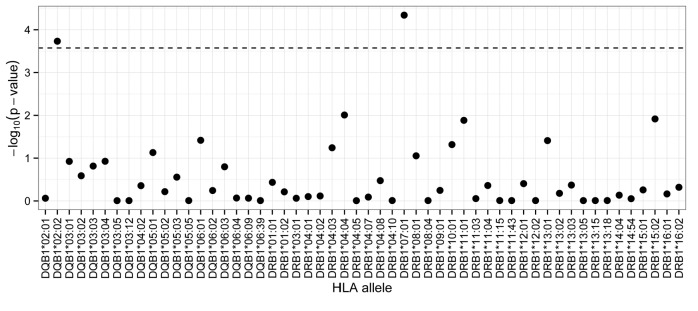
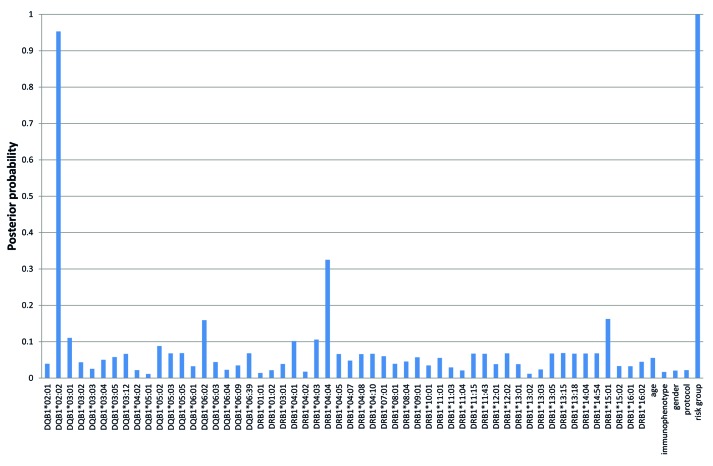
Hypersensitivity reactions are the most frequent dose-limiting adverse reactions to Escherichia coli-derived asparaginase in pediatric acute lymphoblastic leukemia (ALL) patients. The aim of the present study was to identify associations between sequence-based Human Leukocyte Antigen Class II region alleles and asparaginase hypersensitivity in a Hungarian ALL population. Four-digit typing of HLA-DRB1 and HLA-DQB1 loci was performed in 359 pediatric ALL patients by using next-generation sequencing method. Based on genotypic data of the two loci, haplotype reconstruction was carried out. In order to investigate the possible role of the HLA-DQ complex, the HLA-DQA1 alleles were also inferred. Multivariate logistic regression analysis and a Bayesian network-based approach were applied to identify relevant genetic risk factors of asparaginase hypersensitivity. Patients with HLA-DRB1*07:01 and HLA-DQB1*02:02 alleles had significantly higher risk of developing asparaginase hypersensitivity compared to non-carriers [P=4.56×10-5; OR=2.86 (1.73-4.75) and P=1.85×10-4; OR=2.99 (1.68-5.31); n=359, respectively]. After haplotype reconstruction, the HLA-DRB1*07:01-HLA-DQB1*02:02 haplotype was associated with an increased risk. After inferring the HLA-DQA1 alleles the HLA-DRB1*07:01-HLA-DQA1*02:01-HLA-DQB1*02:02 haplotype was associated with the highest risk of asparaginase hypersensitivity [P=1.22×10-5; OR=5.00 (2.43-10.29); n=257]. Significantly fewer T-cell ALL patients carried the HLA-DQB1*02:02 allele and the associated haplotype than did pre-B-cell ALL patients (6.5%; vs. 19.2%, respectively; P=0.047). In conclusion, we identified a haplotype in the Human Leukocyte Antigen Class II region associated with a higher risk of asparaginase hypersensitivity. Our results confirm that variations in HLA-D region might influence the development of asparaginase hypersensitivity.
Copyright© 2017 Ferrata Storti Foundation.
Figures

References
-
- Silverman LB, Gelber RD, Dalton VK, et al. Improved outcome for children with acute lymphoblastic leukemia: results of Dana-Farber Consortium Protocol 91-01. Blood. 2001;97(5):1211–1218. - PubMed
-
- Rizzari C, Conter V, Stary J, et al. Optimizing asparaginase therapy for acute lymphoblastic leukemia. Curr Opin Oncol. 2013;25 Suppl 1:S1–9. - PubMed
-
- Schmiegelow K, Attarbaschi A, Barzilai S, et al. Consensus definitions of 14 severe acute toxic effects for childhood lymphoblastic leukaemia treatment: a Delphi consensus. Lancet Oncol. 2016;17(6):e231–239. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
